
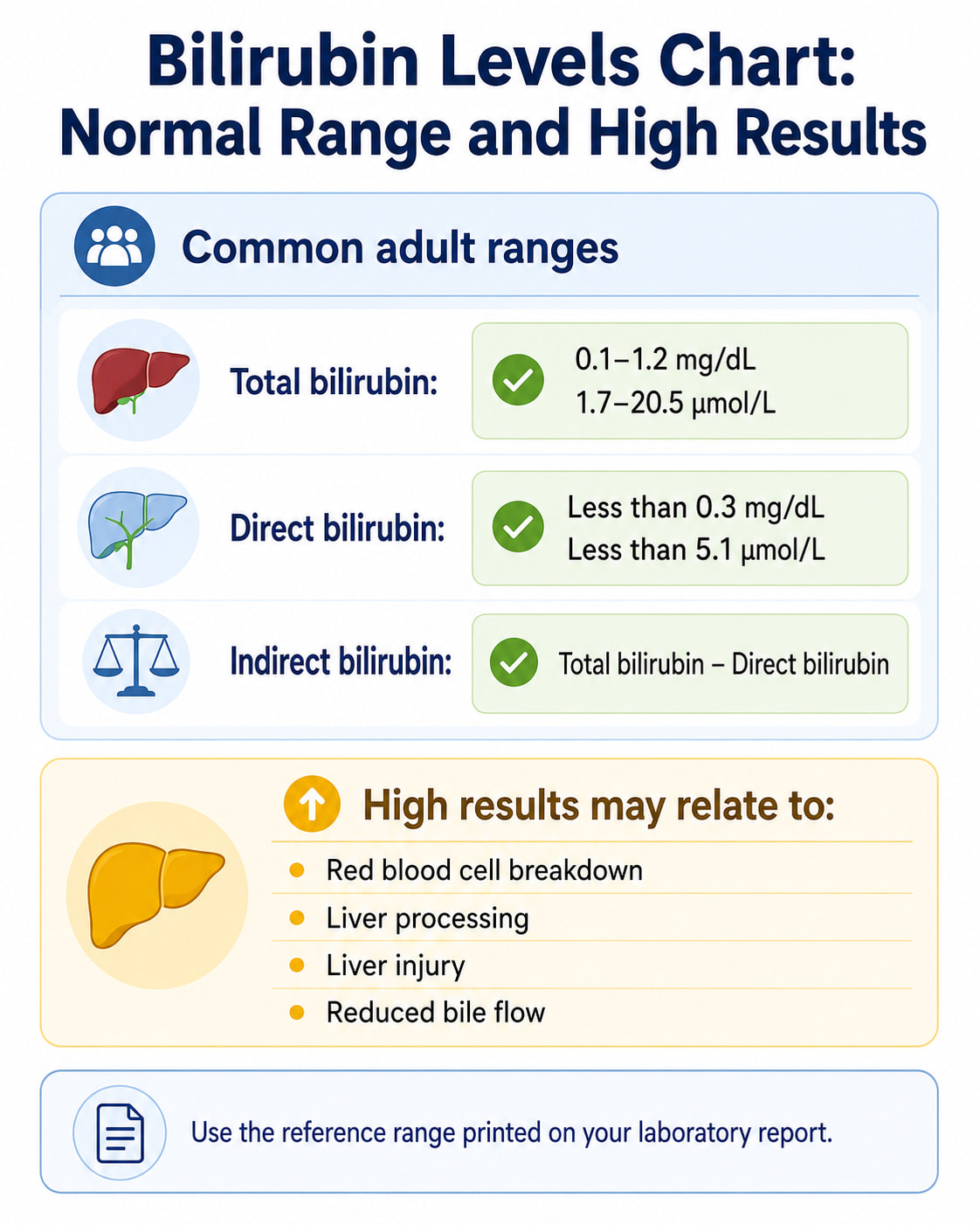
A common normal total bilirubin range for adults is 0.1 to 1.2 mg/dL, while direct bilirubin is usually below 0.3 mg/dL. However, reference ranges vary slightly between laboratories, and a high result must be interpreted according to the type of bilirubin elevated, accompanying symptoms, other blood tests, and the patient’s age.
A bilirubin levels chart can help you understand whether a result falls inside a typical range. It cannot identify the cause of an abnormal result or show how serious the condition is.
Newborn bilirubin levels require a different approach. A baby’s result must be evaluated according to age in hours, gestational age, risk factors, and how quickly the level is changing.
Bilirubin Levels Chart
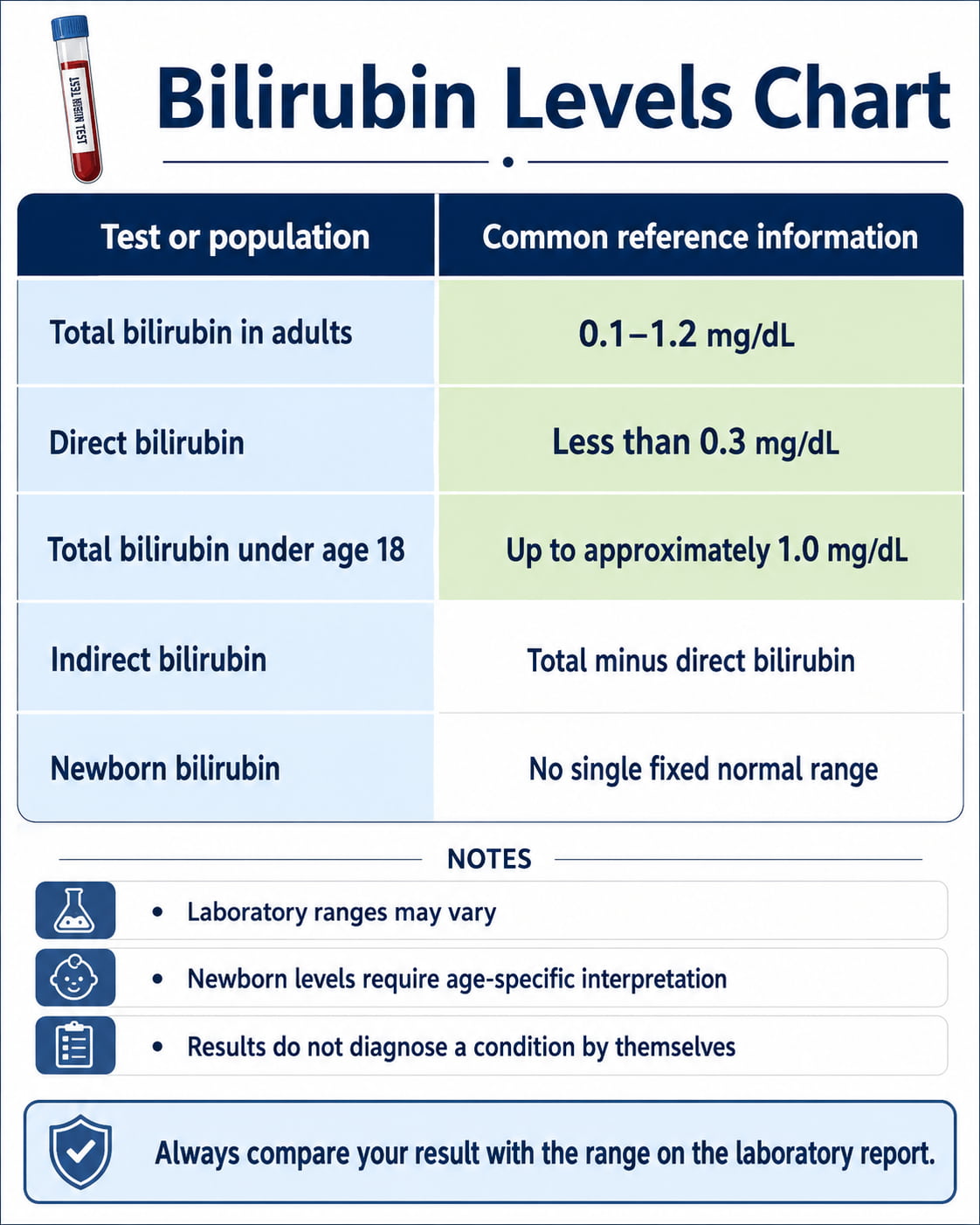
The following bilirubin levels chart shows commonly used blood-test reference ranges. The range printed on your laboratory report should always take priority because testing methods and reference intervals differ.
| Bilirubin test or population | Common reference range | Equivalent in µmol/L | Important note |
|---|---|---|---|
| Total bilirubin in adults | 0.1–1.2 mg/dL | 1.7–20.5 µmol/L | Includes direct and indirect bilirubin |
| Direct bilirubin | Less than 0.3 mg/dL | Less than 5.1 µmol/L | Also called conjugated bilirubin |
| Total bilirubin under age 18 | Up to approximately 1.0 mg/dL | Up to approximately 17.1 µmol/L | Newborns require separate interpretation |
| Indirect bilirubin | Calculated from total minus direct bilirubin | Varies | No single universal range |
| Newborn bilirubin | No single fixed normal range | No single fixed normal range | Must be interpreted by age in hours and clinical risk |
UCSF Health lists a total adult bilirubin range of 0.1–1.2 mg/dL and a direct bilirubin level below 0.3 mg/dL. The institution also emphasizes that normal ranges may vary among laboratories.
Bilirubin Unit Conversion Chart
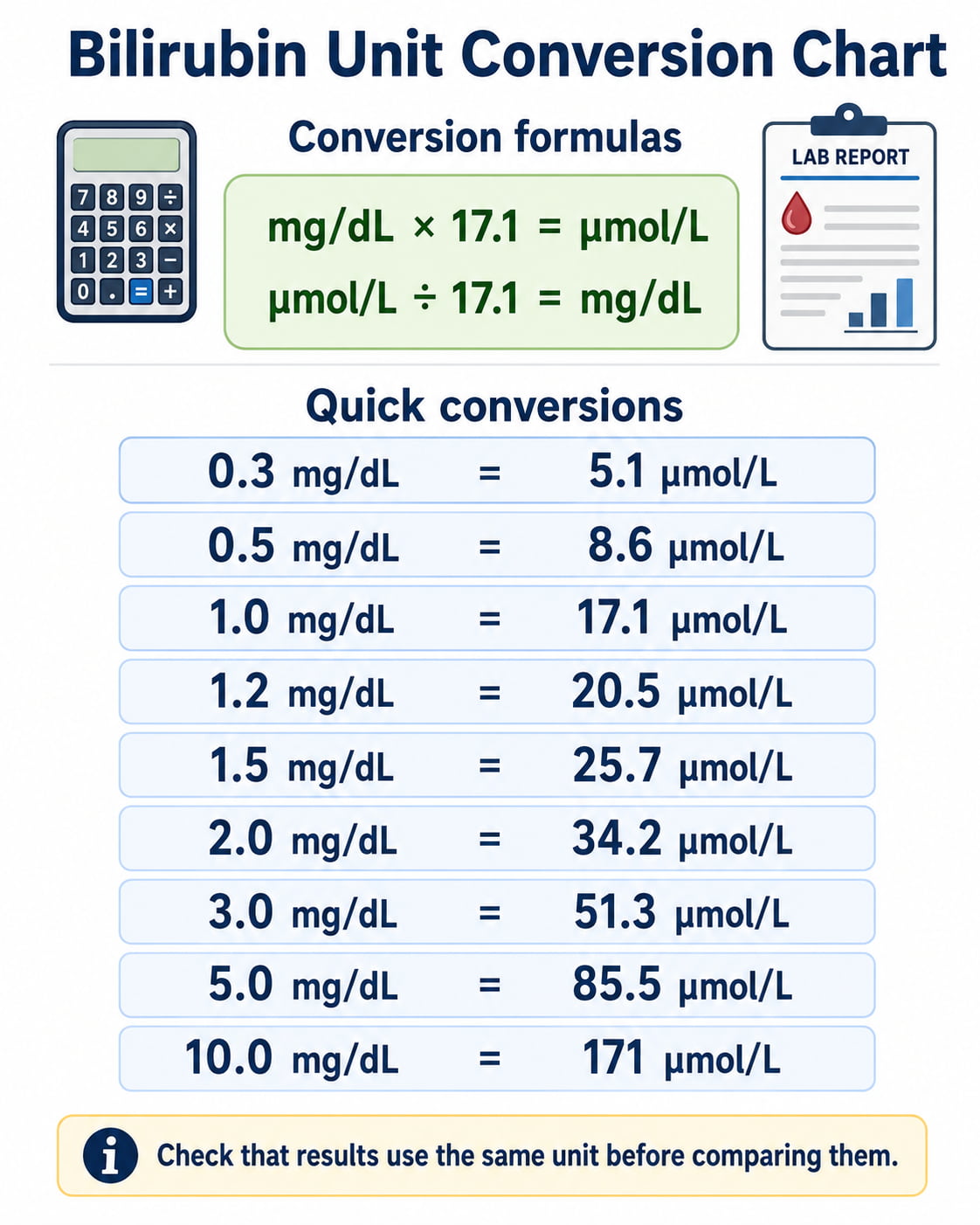
US laboratories commonly report bilirubin in milligrams per deciliter, or mg/dL. Many laboratories outside the United States use micromoles per liter, or µmol/L.
Use these formulas:
- mg/dL × 17.1 = µmol/L
- µmol/L ÷ 17.1 = mg/dL
| Bilirubin in mg/dL | Approximate bilirubin in µmol/L |
|---|---|
| 0.3 mg/dL | 5.1 µmol/L |
| 0.5 mg/dL | 8.6 µmol/L |
| 1.0 mg/dL | 17.1 µmol/L |
| 1.2 mg/dL | 20.5 µmol/L |
| 1.5 mg/dL | 25.7 µmol/L |
| 2.0 mg/dL | 34.2 µmol/L |
| 3.0 mg/dL | 51.3 µmol/L |
| 5.0 mg/dL | 85.5 µmol/L |
| 10.0 mg/dL | 171 µmol/L |
Always confirm that two results use the same unit before comparing them.
What Is Bilirubin?
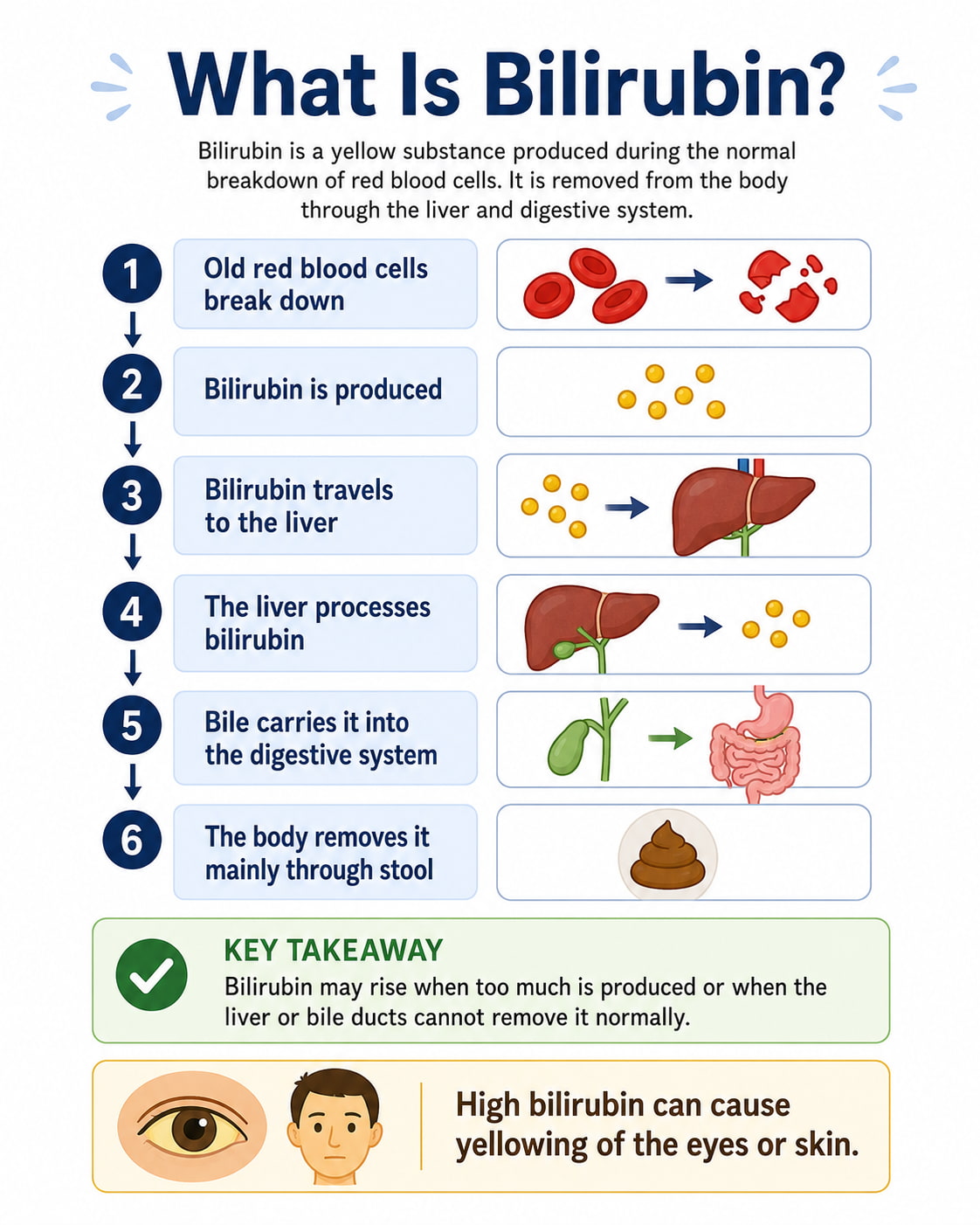
Bilirubin is a yellow-orange substance produced during the normal breakdown of old red blood cells.
Hemoglobin from those cells is broken down into several components, including bilirubin. The bilirubin travels through the bloodstream to the liver, where it is processed and released into bile. Bile then carries it through the digestive system so the body can remove it primarily through stool.
When the body produces more bilirubin than the liver can process—or when the liver or bile ducts cannot remove it normally—bilirubin may accumulate in the blood.
A buildup can cause jaundice, which is a yellow appearance of the skin or whites of the eyes. High bilirubin may result from increased red-blood-cell breakdown, impaired liver processing, liver-cell injury, or reduced bile flow. MedlinePlus explains that bilirubin testing is commonly used to evaluate jaundice, liver health, bile-duct blockage, and newborn jaundice.
Total, Direct, and Indirect Bilirubin
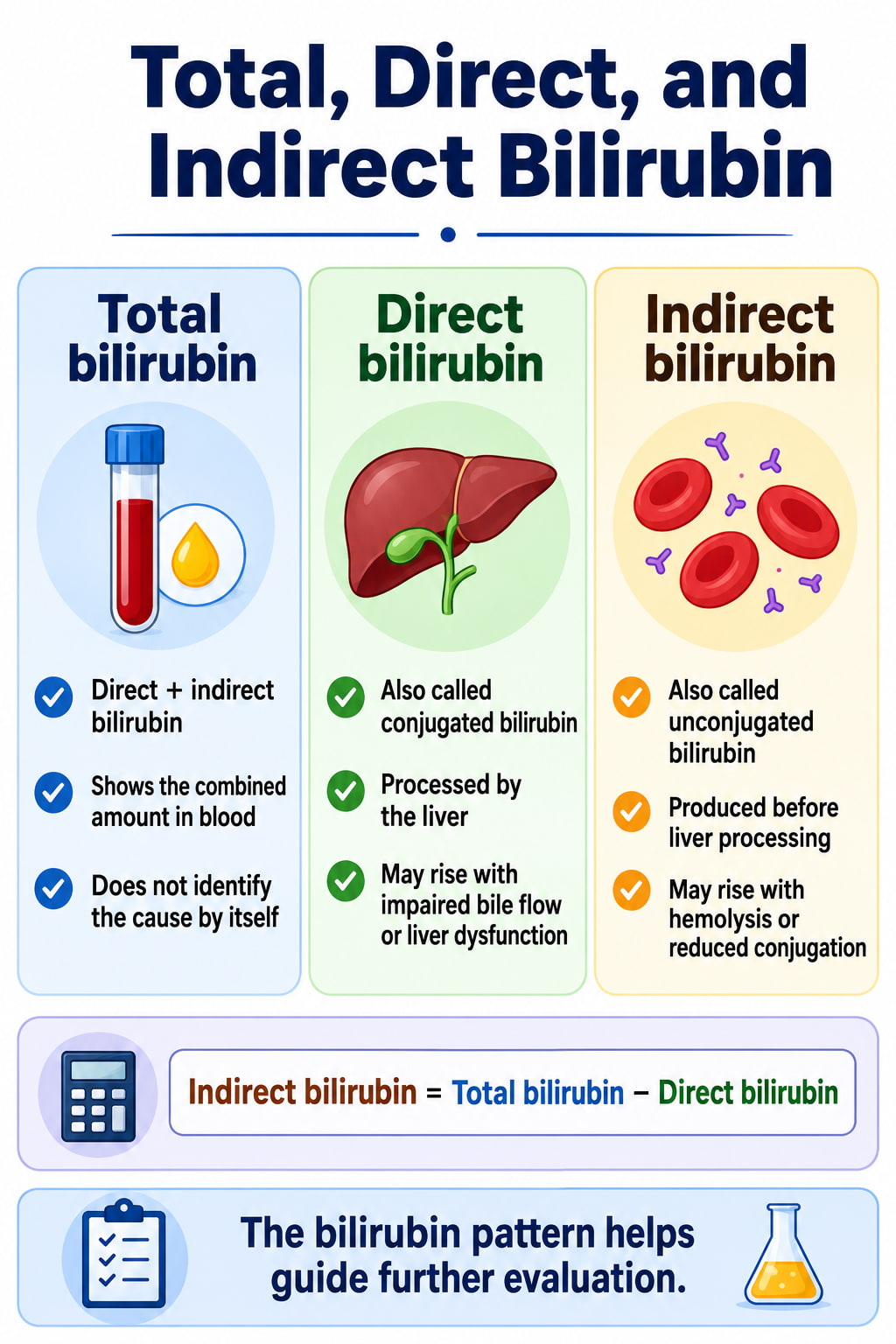
A bilirubin report may contain total bilirubin, direct bilirubin, and indirect bilirubin. Understanding the difference helps explain why two people with similar total results may have different underlying causes.
Total Bilirubin
Total bilirubin measures the combined amount of direct and indirect bilirubin in the blood.
A high total result confirms that bilirubin is elevated, but it does not show why. The direct and indirect components help narrow down the possible source.
Direct Bilirubin
Direct bilirubin is bilirubin that the liver has processed. It is also called conjugated bilirubin.
The liver converts indirect bilirubin into a water-soluble form and releases it into bile. Direct bilirubin may rise when processed bilirubin cannot leave the liver properly.
Possible reasons include:
- Liver-cell injury
- Reduced bile production or flow
- Gallstones
- Narrowing or inflammation of a bile duct
- Cholestasis
- Blockage involving the liver, gallbladder, bile ducts, or pancreas
- Certain inherited disorders
A high direct result does not diagnose a blockage or liver disease by itself.
Indirect Bilirubin
Indirect bilirubin is the form produced before the liver processes it. It is also known as unconjugated bilirubin.
It travels through the bloodstream attached to albumin, a blood protein. Once it reaches the liver, it is converted into direct bilirubin.
Indirect bilirubin is often calculated with this formula:
- Indirect bilirubin = Total bilirubin − Direct bilirubin
Indirect bilirubin may rise because of:
- Increased red-blood-cell destruction
- Hemolytic anemia
- Resorption of a large bruise or hematoma
- Reduced uptake by the liver
- Reduced bilirubin conjugation
- Gilbert syndrome
- Rare inherited conditions such as Crigler–Najjar syndrome
The Mayo Clinic bilirubin blood test guide confirms that indirect bilirubin is calculated by subtracting direct bilirubin from total bilirubin. It also notes that jaundice typically becomes apparent when total bilirubin rises above approximately 3 mg/dL.
Understanding High Bilirubin Results
A bilirubin result is generally considered high when it exceeds the upper limit printed on the laboratory report.
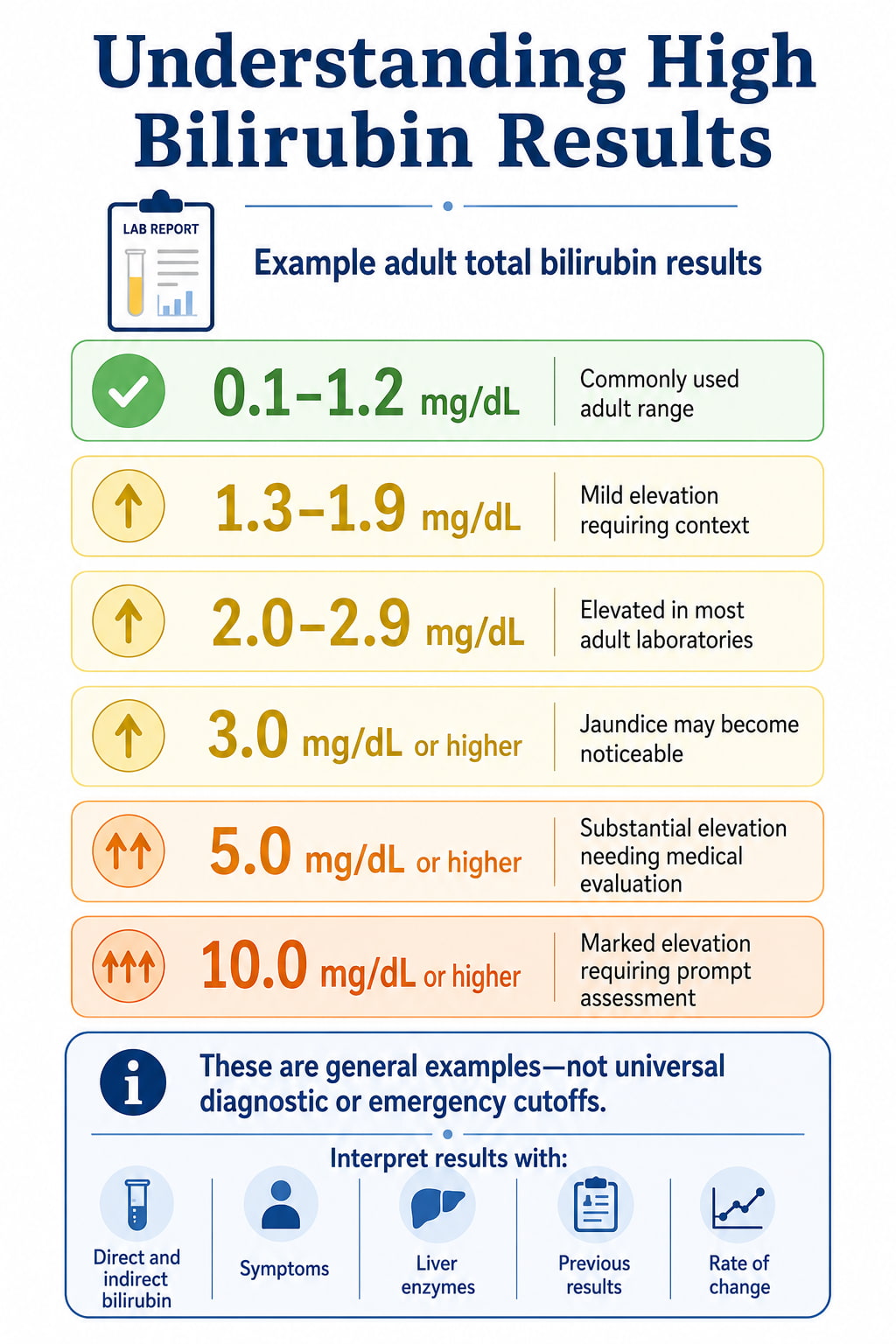
The degree of elevation is only one part of the interpretation. Healthcare professionals also consider:
- Whether direct or indirect bilirubin is elevated
- Whether the value is stable, rising, or falling
- Symptoms
- Liver enzyme results
- Blood counts
- Medications and supplements
- Alcohol use
- Medical history
- Recent illness, fasting, or dehydration
- The patient’s age
The following chart offers general context for adult total bilirubin results. These categories are not diagnostic cutoffs.
| Example adult total bilirubin result | General interpretation |
|---|---|
| 0.1–1.2 mg/dL | Within a commonly used adult range |
| 1.3–1.9 mg/dL | Mild elevation that requires interpretation with the laboratory range and bilirubin type |
| 2.0–2.9 mg/dL | Clearly elevated in most adult laboratories; further evaluation may be appropriate |
| 3.0 mg/dL or higher | Jaundice may become noticeable; the cause and symptoms determine urgency |
| 5.0 mg/dL or higher | Substantial elevation that should be medically evaluated |
| 10.0 mg/dL or higher | Marked elevation requiring prompt assessment, especially with symptoms |
These values should not be used to diagnose a condition or decide whether medical care is necessary. Someone with a modest increase and severe symptoms may require more urgent attention than someone with a higher, stable level from a known condition.
Is a Bilirubin Level of 1.5 High?
A total bilirubin level of 1.5 mg/dL is slightly above the upper limit used by many adult laboratories.
Possible explanations include:
- Temporary laboratory variation
- Gilbert syndrome
- Recent fasting
- Dehydration
- Illness
- Increased red-blood-cell breakdown
- A liver or bile-flow problem
- A medication effect
The direct and indirect results are important. For example, an isolated indirect elevation with otherwise normal liver enzymes may suggest a different group of causes than a high direct result accompanied by increased alkaline phosphatase.
A single result of 1.5 mg/dL usually does not establish a diagnosis. A healthcare professional may compare it with previous results or repeat the test.
What Does a Bilirubin Level of 2.0 Mean?
A total bilirubin level of 2.0 mg/dL is elevated according to most adult reference ranges.
Some people may have no visible symptoms at this level. Others may notice a subtle yellow appearance in the whites of the eyes.
The meaning depends on:
- The percentage that is direct or indirect
- Other liver-test results
- Whether the level is new
- Whether it is rising
- The presence of pain, fever, dark urine, pale stool, fatigue, or other symptoms
A result of 2.0 mg/dL may occur with a relatively harmless condition such as Gilbert syndrome, but it can also occur with hemolysis, hepatitis, medication-related injury, or impaired bile flow. It should not be interpreted from the number alone.
What Does a Bilirubin Level of 3.0 Mean?
A total bilirubin level of 3.0 mg/dL is significantly above the common adult range.
Jaundice often becomes visible around this level or higher, particularly in the whites of the eyes. However, the visibility of jaundice varies with lighting, skin tone, and the speed at which the bilirubin increased.
A new level of 3.0 mg/dL should be discussed with a healthcare professional. Prompt assessment is especially important when it occurs with:
- Abdominal pain
- Fever
- Vomiting
- Dark urine
- Pale or gray stool
- Confusion
- Unusual bleeding
- Rapidly worsening yellowing
What Level of Bilirubin Is Dangerous?
There is no single bilirubin number that is considered dangerous for every adult.
The risk depends mainly on the cause of the elevation and whether the liver is functioning normally. The same bilirubin value may have different implications in someone with Gilbert syndrome, acute hepatitis, a blocked bile duct, hemolysis, or advanced liver disease.
Healthcare professionals evaluate the result together with:
- ALT and AST
- Alkaline phosphatase
- GGT
- Albumin
- Prothrombin time or INR
- Complete blood count
- Symptoms and physical findings
- Imaging results when appropriate
A rapidly increasing result may be more concerning than a stable result. Severe symptoms can also make a lower bilirubin level urgent.
Newborns are different. Very high unconjugated bilirubin can enter brain tissue and cause bilirubin encephalopathy or kernicterus. Because newborn risk depends on age in hours and other factors, an adult bilirubin chart must never be used for a baby.
High Direct vs. High Indirect Bilirubin
The bilirubin pattern can help organize the possible causes.
| Bilirubin pattern | Possible explanations |
|---|---|
| Mostly indirect bilirubin | Hemolysis, Gilbert syndrome, reduced liver uptake, reduced conjugation, large hematoma |
| Mostly direct bilirubin | Cholestasis, bile-duct obstruction, impaired bile excretion, liver-cell dysfunction |
| Both direct and indirect elevated | Hepatitis, medication-related liver injury, cirrhosis, severe illness, mixed liver or bile-duct disorders |
According to the MSD Manual Professional Edition, predominantly unconjugated hyperbilirubinemia generally results from increased production, decreased liver uptake, or decreased conjugation. Predominantly conjugated hyperbilirubinemia is more often related to liver-cell dysfunction, intrahepatic cholestasis, or obstruction of bile flow outside the liver.
High Indirect Bilirubin With Normal Liver Enzymes
An isolated indirect bilirubin elevation with normal ALT, AST, and alkaline phosphatase may occur with Gilbert syndrome. This inherited condition reduces the liver’s ability to process bilirubin efficiently.
Bilirubin can fluctuate in people with Gilbert syndrome. Potential triggers include:
- Fasting
- A very low-calorie diet
- Dehydration
- Illness
- Stress
- Menstruation
- Strenuous exercise
Gilbert syndrome is generally considered harmless and usually does not require treatment. However, similar patterns can occur with hemolysis and other conditions, so it should not be self-diagnosed solely from an online chart.
A healthcare professional may review blood counts and other markers to exclude increased red-blood-cell breakdown.
High Direct Bilirubin With Normal or Abnormal Liver Enzymes
A high direct bilirubin level may indicate difficulty moving processed bilirubin from the liver into the digestive tract.
Possible causes include:
- Gallstones
- Bile-duct narrowing
- Cholestasis
- Hepatitis
- Medication-related liver injury
- Cirrhosis
- Gallbladder inflammation
- Pancreatic or bile-duct disorders
Direct bilirubin may rise before, with, or after changes in other liver tests. The complete pattern is more useful than one result.
Common Causes of High Bilirubin
High bilirubin can develop through several different mechanisms.
Increased Red-Blood-Cell Breakdown
When red blood cells break down faster than normal, the body produces more indirect bilirubin.
Possible causes include:
- Hemolytic anemia
- Sickle cell disease
- Certain inherited red-blood-cell conditions
- Blood-transfusion reactions
- Blood-type incompatibility in newborns
- Resorption of a large bruise
- Some infections or medications
Other blood tests may be needed to determine whether hemolysis is occurring.
Reduced Bilirubin Processing
The liver may receive bilirubin normally but have difficulty taking it up or converting it into its direct form.
Possible causes include:
- Gilbert syndrome
- Crigler–Najjar syndrome
- Certain medications
- Severe illness
- Immature liver function in newborns
Liver-Cell Injury
Conditions that damage or inflame liver cells can interfere with bilirubin processing and excretion.
Examples include:
- Viral hepatitis
- Autoimmune hepatitis
- Alcohol-related liver disease
- Metabolic dysfunction-associated steatotic liver disease
- Cirrhosis
- Medication-related liver injury
- Toxin exposure
- Severe infection
These conditions often affect other liver tests, although the pattern varies.
Reduced Bile Flow
Processed bilirubin normally leaves the liver through bile. A blockage or reduction in bile flow may increase direct bilirubin.
Possible causes include:
- Gallstones
- Bile-duct strictures
- Inflammation of the bile ducts
- Cholestasis
- Pancreatitis
- Masses affecting the pancreas, gallbladder, liver, or bile ducts
- Biliary atresia in infants
Dark urine and pale or clay-colored stool are particularly important symptoms because they may occur when conjugated bilirubin cannot flow normally into the intestine.
Can Dehydration Raise Bilirubin?
Dehydration may contribute to a temporary bilirubin increase, particularly in people with Gilbert syndrome.
Dehydration can also make blood more concentrated. However, it should not automatically be assumed to explain an abnormal result. Persistent or substantial elevations require appropriate medical interpretation.
Drinking water does not correct bilirubin caused by hepatitis, hemolysis, gallstones, bile-duct obstruction, or another underlying disorder.
Can Fasting Raise Bilirubin?
Fasting or severe calorie restriction may raise indirect bilirubin, especially in someone with Gilbert syndrome.
Tell your healthcare professional if you:
- Fasted before the test
- Were unable to eat because of illness
- Recently followed a very low-calorie diet
- Were dehydrated
- Completed strenuous exercise
- Had a recent infection
This information can help with interpretation, but it does not replace an appropriate evaluation.
Symptoms That May Occur With High Bilirubin
Some people with mild bilirubin elevation have no symptoms. When symptoms occur, they may include:
- Yellowing of the whites of the eyes
- Yellowing of the skin
- Dark brown or orange urine
- Pale, gray, or clay-colored stool
- Itching
- Fatigue
- Reduced appetite
- Nausea or vomiting
- Abdominal pain
- Fever or chills
- Unexplained weight loss
Symptoms depend on the cause. For example, a bile-duct obstruction may cause abdominal pain, dark urine, pale stool, and itching. Hemolysis may cause weakness, pallor, or shortness of breath. Hepatitis may cause fatigue, nausea, discomfort, or jaundice.
When to Seek Medical Care
Contact a healthcare professional promptly for new or worsening jaundice.
Urgent assessment is particularly important when yellow skin or eyes occur with:
- Fever or chills
- Severe or worsening abdominal pain
- Repeated vomiting
- Confusion, extreme sleepiness, or behavior changes
- Fainting
- Unusual bleeding or easy bruising
- Black or bloody stool
- Significant weakness
- Very dark urine
- Pale or white stool
- Rapidly worsening symptoms
These signs may indicate a serious liver, gallbladder, bile-duct, pancreatic, blood, or systemic condition.
Bilirubin Levels Chart for Newborns
There is no single normal or dangerous bilirubin level that applies to every newborn.
Newborn bilirubin must be interpreted according to:
- Exact age in hours
- Gestational age at birth
- Total serum bilirubin
- Rate of increase
- Feeding and hydration
- Prematurity
- Red-blood-cell breakdown
- Infection or clinical instability
- Albumin level
- Other neurotoxicity risk factors
- Distance from the phototherapy threshold
The current American Academy of Pediatrics hyperbilirubinemia guidance applies to infants born at 35 or more weeks of gestation. Released in August 2022, it remains valid through August 2027. Treatment and follow-up decisions are based on hour-specific bilirubin levels, gestational age, and risk factors rather than a single universal cutoff.
Why Newborn Bilirubin Levels Rise
Bilirubin commonly rises during the first few days after birth because:
- Newborns break down more red blood cells
- Their livers are still developing
- Bilirubin may be reabsorbed through the intestines
- Feeding may not yet be well established
Many babies develop mild jaundice that improves without treatment. However, a rapidly increasing or very high unconjugated bilirubin level can be harmful.
When Should a Newborn Be Tested?
The American Academy of Pediatrics recommends that:
- A baby with jaundice during the first 24 hours have bilirubin measured promptly.
- Every newborn have at least one bilirubin measurement before hospital discharge.
- Follow-up timing be based on the bilirubin level, age, gestational age, and relevant risks.
- Babies discharged early receive timely follow-up after leaving the hospital.
Parents should ask what their baby’s bilirubin level was before discharge and when it should be checked again.
Newborn Warning Signs
Contact the baby’s healthcare professional promptly when:
- Jaundice appears during the first 24 hours
- Yellowing becomes more intense
- Yellowing spreads to the abdomen, arms, or legs
- The baby is difficult to wake
- The baby is unusually fussy
- Feeding is poor
- The baby produces fewer wet diapers
- The baby has a fever
- Urine is unusually dark
- Stool is pale, gray, or white
Very high newborn bilirubin is a medical emergency. Phototherapy is a common medical intervention when treatment is required. Sunlight is not considered a safe substitute for medically supervised phototherapy.
Important Direct Bilirubin Guidance for Infants
A 2025 American Academy of Pediatrics clinical report introduced an updated strategy for recognizing biliary atresia by two to four weeks of age.
Before two weeks of age, direct or conjugated bilirubin should be compared with the specific laboratory’s reference interval. A fixed cutoff or percentage should not be used during this early period.
At two to four weeks, a direct or conjugated bilirubin level of 1 mg/dL or higher warrants urgent consultation with a pediatric gastroenterologist.
Testing should be considered when:
- The baby’s eyes or skin remain yellow
- Stool is pale, gray, or white
- A previous direct bilirubin result exceeded the laboratory range
The AAP clinical report on identifying biliary atresia also emphasizes that even a small elevation above the laboratory’s range before two weeks can be meaningful.
How a Bilirubin Blood Test Is Performed
For adults and older children, blood is usually drawn from a vein in the arm.
For newborns, testing may involve:
- A heel-stick blood sample
- A venous blood sample
- A transcutaneous bilirubin meter placed against the skin
A transcutaneous reading estimates bilirubin without drawing blood. A blood test may still be needed when the result is high, close to a treatment threshold, or inconsistent with the baby’s condition.
Do You Need to Fast for a Bilirubin Test?
Many bilirubin tests require no special preparation.
However, fasting instructions can depend on:
- The other blood tests ordered
- The laboratory
- Medications
- The reason for testing
Follow the instructions from the healthcare professional or laboratory. Do not stop a prescription medicine unless the prescribing professional specifically recommends it.
Tell the healthcare professional about:
- Prescription medicines
- Over-the-counter medicines
- Vitamins
- Herbal products
- Alcohol use
- Recent fasting
- Dehydration
- Recent strenuous exercise
- Current illness
What Other Tests May Be Ordered?
A bilirubin result is often evaluated with additional tests.
These may include:
- ALT
- AST
- Alkaline phosphatase
- GGT
- Albumin
- Total protein
- Prothrombin time or INR
- Complete blood count
- Reticulocyte count
- LDH
- Haptoglobin
- Viral hepatitis tests
- Urinalysis
An ultrasound or another imaging test may be considered when a gallstone, bile-duct obstruction, or structural problem is suspected.
The appropriate tests depend on the bilirubin pattern, symptoms, examination findings, and medical history.
How Is High Bilirubin Managed?
There is no single treatment for elevated bilirubin. Management focuses on the underlying cause.
Depending on the diagnosis, care may involve:
- Monitoring a mild, stable elevation
- Reviewing medications
- Managing a liver condition
- Evaluating increased red-blood-cell breakdown
- Removing a bile-duct obstruction
- Treating an infection
- Providing newborn feeding support
- Using phototherapy for newborn jaundice
- Providing intensive hospital care for severe neonatal hyperbilirubinemia
Do not rely on detox drinks, restrictive diets, herbs, or supplements to lower bilirubin. Some supplements can injure the liver or interact with medications.
Frequently Asked Questions
What is a normal bilirubin level for adults?
A commonly used total bilirubin range is 0.1–1.2 mg/dL. Direct bilirubin is commonly below 0.3 mg/dL. Always use the reference interval on the actual laboratory report.
Is a bilirubin level of 1.5 mg/dL high?
Yes. A total bilirubin level of 1.5 mg/dL is slightly above the common adult upper limit of 1.2 mg/dL. It may be temporary or related to Gilbert syndrome, hemolysis, liver conditions, medications, fasting, or dehydration. The direct and indirect results provide additional context.
Is a bilirubin level of 2.0 mg/dL serious?
A level of 2.0 mg/dL is elevated, but the number alone cannot show whether the cause is serious. It should be interpreted with symptoms, direct and indirect bilirubin, other liver tests, and previous results.
At what bilirubin level does jaundice appear?
According to Mayo Clinic, jaundice typically becomes noticeable when total bilirubin is above approximately 3 mg/dL. Visibility varies among people and may be harder to assess in some skin tones or lighting conditions. Yellowing of the whites of the eyes may be easier to recognize.
What does high bilirubin with normal liver enzymes mean?
An isolated indirect bilirubin elevation with otherwise normal liver tests may occur with Gilbert syndrome. Hemolysis and other causes must sometimes be excluded. A healthcare professional may review blood counts and additional tests before making a diagnosis.
Is low bilirubin dangerous?
Low bilirubin generally is not considered a medical concern. The test is primarily used to investigate elevated values. The result should still be interpreted with the laboratory’s reference range and the reason testing was ordered.
What is a dangerous bilirubin level in a newborn?
There is no single dangerous cutoff for every newborn. Risk depends on the baby’s exact age in hours, gestational age, bilirubin trend, clinical condition, and neurotoxicity risk factors. A baby’s result should be evaluated with the current AAP hour-specific guidance.
Conclusion
A bilirubin levels chart provides a useful starting point for reading a laboratory report. For most adults, total bilirubin is commonly 0.1–1.2 mg/dL, while direct bilirubin is usually below 0.3 mg/dL.
A result above these values does not identify a specific disease. The most useful clues are whether direct or indirect bilirubin is elevated, whether the level is changing, and whether symptoms or other laboratory abnormalities are present.
New or worsening jaundice should be medically evaluated. Newborn results require prompt age-specific interpretation and should never be assessed with an adult chart.
Discuss an abnormal result with a qualified healthcare professional rather than using the bilirubin number alone to make health decisions.
This content is for informational purposes only and not medical advice.