
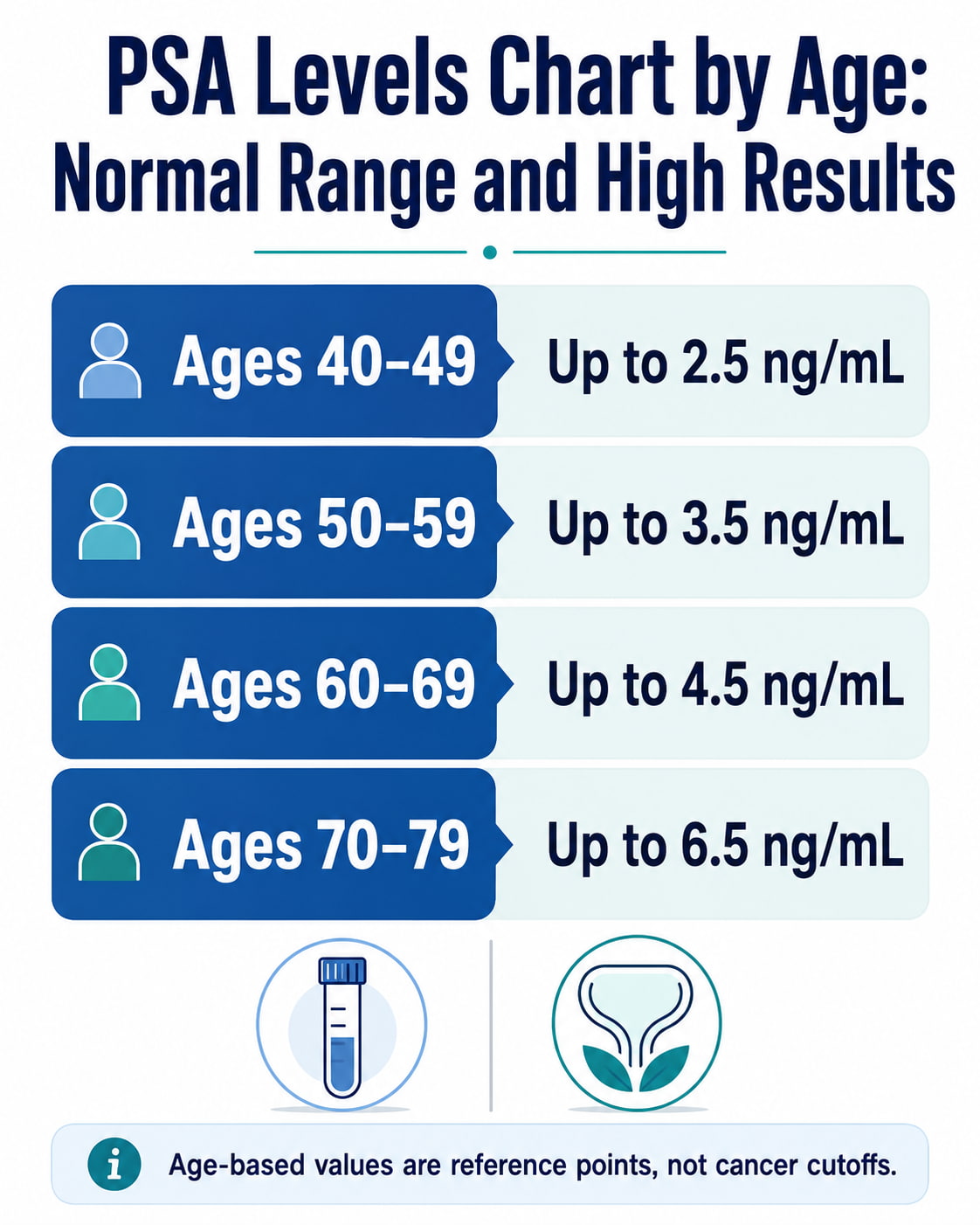
Commonly cited upper PSA reference levels are 2.5 ng/mL for ages 40–49, 3.5 ng/mL for ages 50–59, 4.5 ng/mL for ages 60–69, and 6.5 ng/mL for ages 70–79. However, these age-based values are reference points—not universal cancer cutoffs.
A high prostate-specific antigen result does not automatically mean you have prostate cancer. Benign prostate enlargement, inflammation, infection, ejaculation, cycling, medications, and recent medical procedures can also affect PSA.
The National Cancer Institute explains that there is no single PSA threshold that reliably separates a normal result from an abnormal one. Your age, previous results, prostate size, symptoms, medications, family history, overall health, and laboratory reference range all matter.
PSA Levels Chart by Age
The following PSA levels chart by age shows traditional age-adjusted reference ranges. These values were developed as approximate upper reference limits among men without clinically evident prostate cancer.
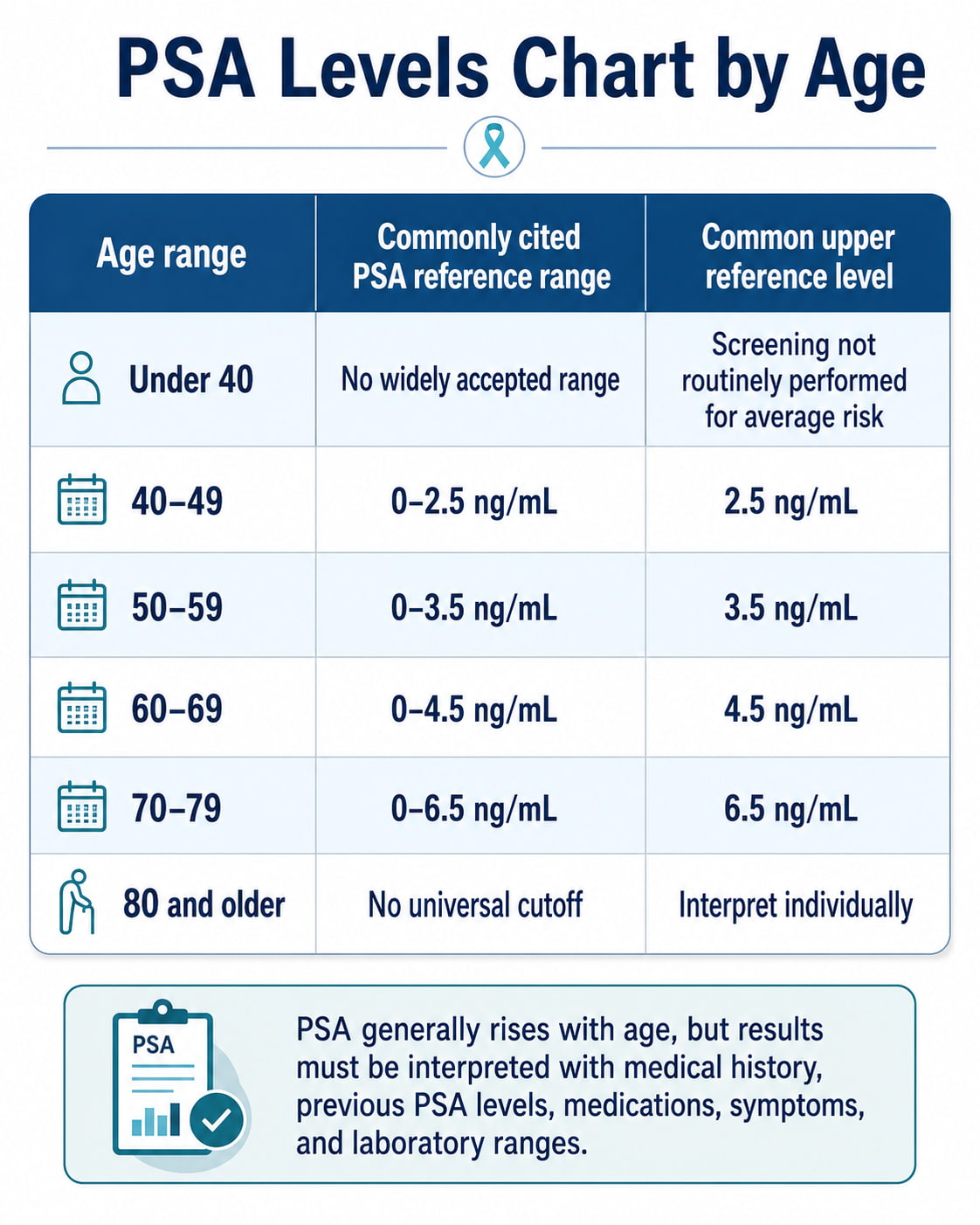
| Age range | Commonly cited PSA reference range | Common upper reference level |
|---|---|---|
| Under 40 | No widely accepted age-specific range | Screening is not routinely performed in average-risk adults |
| 40–49 | 0–2.5 ng/mL | 2.5 ng/mL |
| 50–59 | 0–3.5 ng/mL | 3.5 ng/mL |
| 60–69 | 0–4.5 ng/mL | 4.5 ng/mL |
| 70–79 | 0–6.5 ng/mL | 6.5 ng/mL |
| 80 and older | No universal cutoff | Interpret individually |
These traditional values originated from age-specific reference research published in the 1990s. They represent approximate 95th-percentile limits, not levels that can confirm or exclude prostate cancer.
Important Note About the PSA Chart
A result inside the age-based range does not guarantee that prostate cancer is absent. A result above the range does not prove that cancer is present.
The American Cancer Society notes that the usefulness of age-specific PSA ranges has not been firmly established. Many doctors and professional organizations therefore do not recommend using an age-based cutoff as the only basis for further testing.
Updated Research on Age-Adjusted PSA Ranges
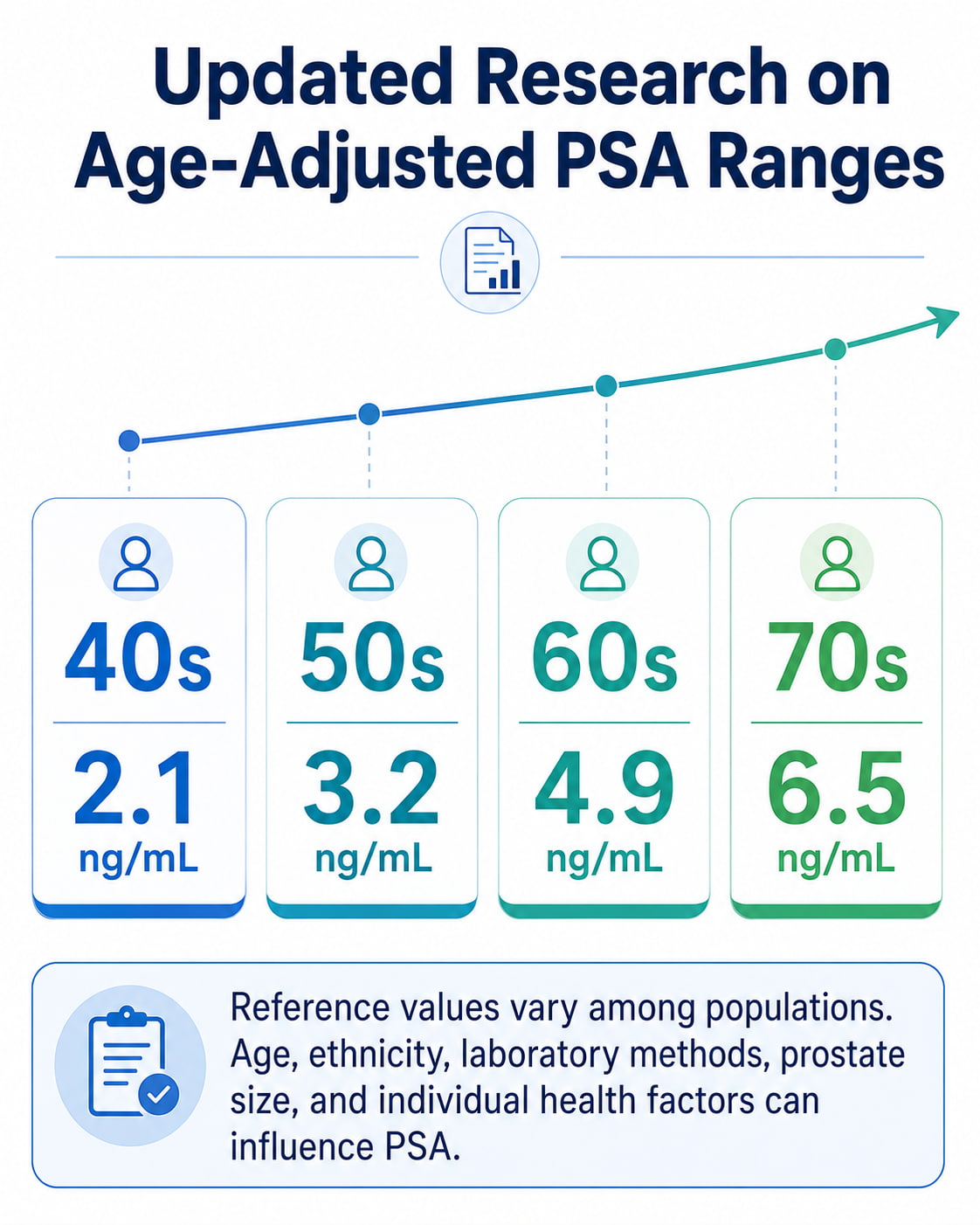
A 2022 systematic review and meta-analysis reported the following pooled upper reference limits:
| Age decade | Pooled upper PSA reference limit |
|---|---|
| 40s | 2.1 ng/mL |
| 50s | 3.2 ng/mL |
| 60s | 4.9 ng/mL |
| 70s | 6.5 ng/mL |
The researchers found considerable variation among populations. Age and ethnicity contributed to differences in PSA reference values, which is another reason not to treat one chart as a universal diagnostic standard.
What Is a PSA Test?
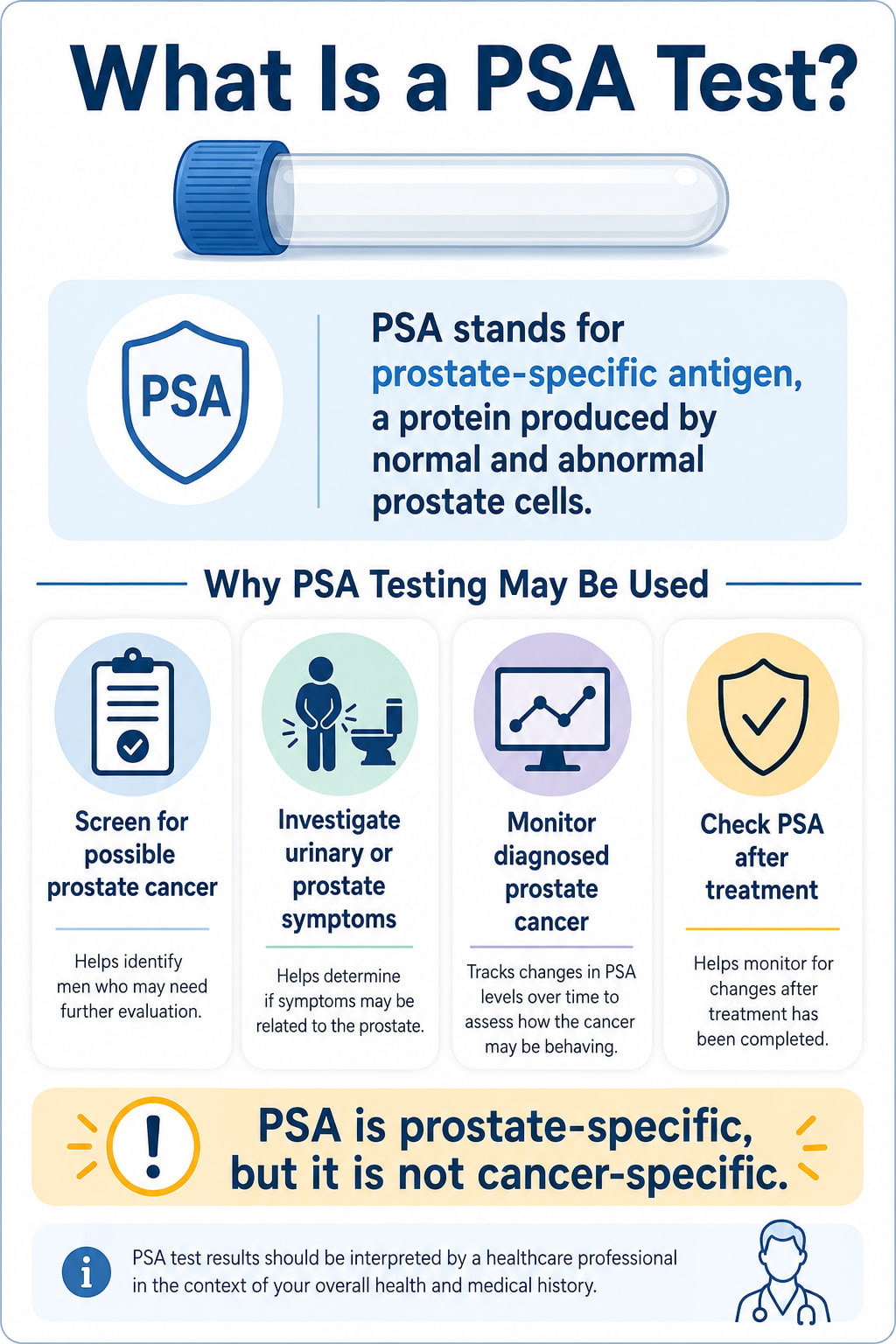
PSA stands for prostate-specific antigen. It is a protein produced by both normal and abnormal cells in the prostate gland.
A small amount of PSA normally circulates in the blood. A PSA blood test measures that amount in nanograms per milliliter, written as ng/mL.
Doctors may use PSA testing to:
- Screen for possible prostate cancer before symptoms develop
- Investigate urinary or prostate-related symptoms
- Help assess an abnormal prostate examination
- Monitor someone who has already been diagnosed with prostate cancer
- Check for recurrence after prostate cancer treatment
PSA is prostate-specific, but it is not cancer-specific. Benign prostatic hyperplasia, prostatitis, prostate cancer, and other factors can all increase the result.
What Is Considered a Normal PSA Level?
There is no single normal PSA level that applies to every person.
Historically, a PSA result below 4.0 ng/mL was commonly described as normal. Today, clinicians recognize that this approach is too simple.
Some people with PSA levels below 4.0 ng/mL have prostate cancer. Many people with levels above 4.0 ng/mL do not have cancer. Doctors may also consider lower thresholds, such as 2.5 or 3.0 ng/mL, in younger adults or people with additional risk factors.
A PSA result is generally interpreted using:
- Your age
- Your current laboratory’s reference range
- Earlier PSA results
- How quickly the level has changed
- Prostate size
- Digital rectal examination findings
- Urinary or pelvic symptoms
- Family history of prostate cancer
- Black ancestry
- Known inherited genetic variants
- Current medications
- Recent infections or procedures
- Overall health and estimated life expectancy
A clinician may be more concerned about a PSA of 4.0 ng/mL in a healthy 50-year-old than the same level in an 80-year-old with a significantly enlarged prostate. The number must always be considered in context.
PSA Levels Chart: What High Results May Mean
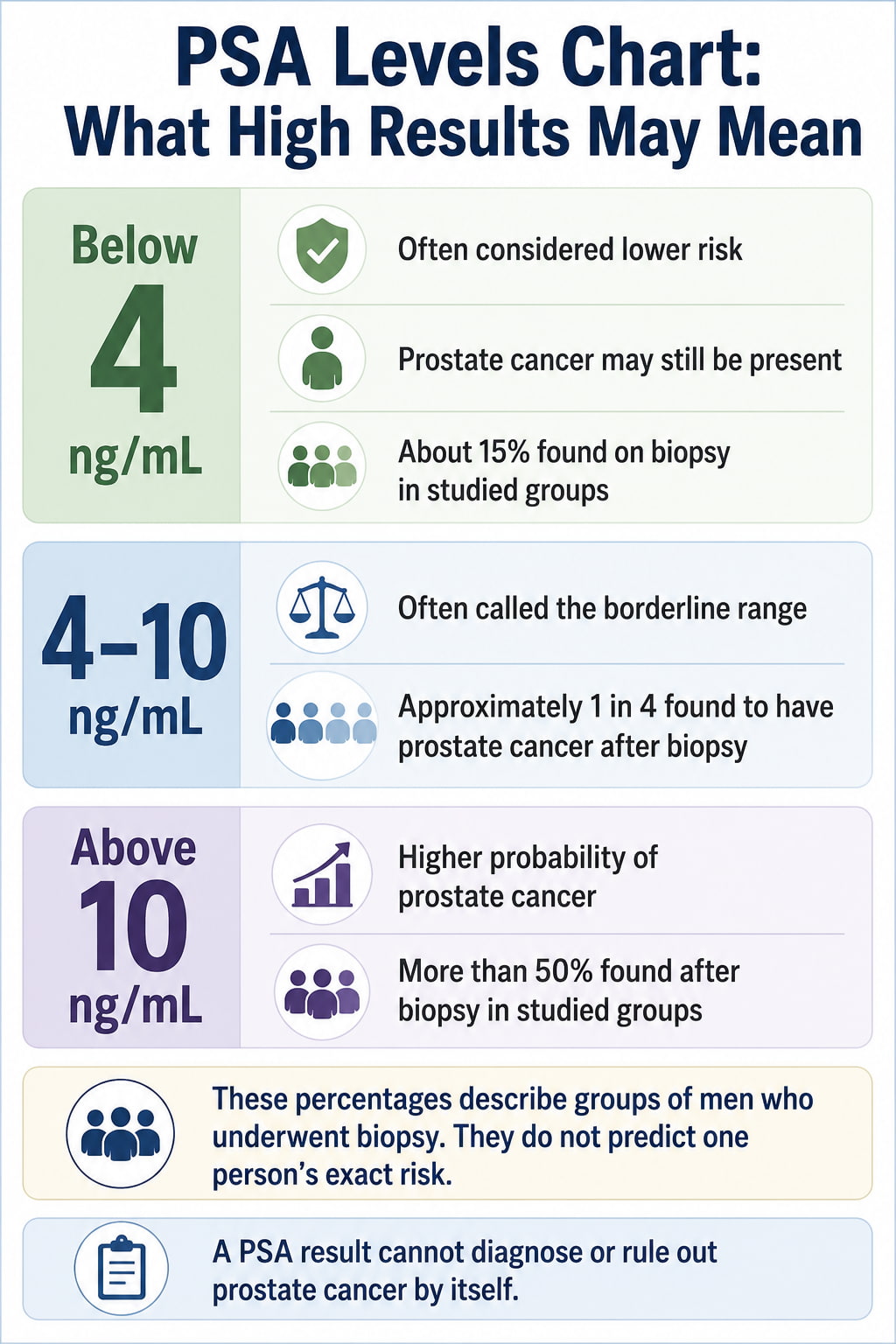
The following ranges provide general context for an initial screening result. They do not diagnose prostate cancer.
| Total PSA result | General interpretation | Approximate cancer probability reported by the ACS |
|---|---|---|
| Below 4 ng/mL | Often considered a lower-risk range, but cancer remains possible | About 15% if a biopsy is performed |
| 4–10 ng/mL | Often called the borderline range | About 1 in 4 |
| Above 10 ng/mL | Higher probability of prostate cancer | More than 50% |
The percentages above describe population-level findings. They cannot predict an individual person’s exact risk. The American Cancer Society’s PSA testing guidance emphasizes that there is no set cutoff that can determine with certainty whether prostate cancer is present.
PSA Below 4 ng/mL
A result below 4 ng/mL is often reassuring, particularly when it is stable and consistent with previous test results.
However, a PSA below 4 does not completely rule out prostate cancer. The ACS reports that about 15% of men with PSA below 4 who undergo biopsy are found to have prostate cancer.
The individual risk may be influenced by:
- Age
- Family history
- Black ancestry
- Genetic risk
- Prostate examination findings
- PSA trend
- Prostate size
- Other blood, urine, or imaging results
PSA Between 4 and 10 ng/mL
A PSA level from 4 to 10 ng/mL is often called the borderline or gray-zone range.
Approximately one in four men in this range is found to have prostate cancer. This also means that most people with a PSA between 4 and 10 do not have cancer.
Doctors commonly consider temporary causes of elevation before recommending invasive testing. A repeat PSA, percent-free PSA, risk calculator, biomarker test, prostate MRI, or digital rectal examination may provide more information.
PSA Above 10 ng/mL
A PSA above 10 ng/mL is associated with a higher probability of prostate cancer. The ACS estimates that the chance exceeds 50% at this level.
Even so, PSA above 10 does not provide a diagnosis by itself. Severe prostate inflammation, infection, urinary problems, recent prostate procedures, and substantial benign enlargement may also cause high values.
A result in this range generally deserves timely medical follow-up.
Is There a Dangerous PSA Level?
There is no single PSA number at which the result automatically becomes “dangerous.”
In general, concern increases as PSA rises, particularly when:
- The result remains high on repeat testing
- PSA has increased substantially from previous results
- A digital rectal examination is abnormal
- Prostate MRI identifies a suspicious area
- The person has a strong family history
- The person has Black ancestry or a relevant inherited mutation
- Urinary, pelvic, or systemic symptoms are present
A very high result may lead to more urgent evaluation, but PSA still cannot determine the diagnosis, cancer grade, or cancer stage by itself.
Do not assume that a high result means cancer. Do not delay follow-up because the result is only slightly elevated. The appropriate next step depends on the entire clinical picture.
Common Causes of High PSA Other Than Cancer
Several noncancerous conditions and temporary factors can increase PSA.
Benign Prostatic Hyperplasia
Benign prostatic hyperplasia, or BPH, is a noncancerous enlargement of the prostate.
As the prostate becomes larger, it can produce more PSA. BPH becomes more common with age and may cause:
- A weak urine stream
- Difficulty starting urination
- Frequent urination
- A feeling that the bladder has not emptied
- Increased nighttime urination
BPH does not cause prostate cancer, although a person can have both conditions at the same time.
Prostatitis
Prostatitis is inflammation of the prostate. It may occur with or without a bacterial infection.
Prostatitis can cause a substantial temporary rise in PSA. Possible symptoms include:
- Painful urination
- Pelvic discomfort
- Urinary frequency
- Fever or chills
- Pain during ejaculation
Testing may need to be delayed until inflammation or infection has resolved.
Increasing Age
PSA commonly rises gradually with age, even when cancer is not present. Part of this increase may be related to normal prostate growth and the higher prevalence of BPH in older adults.
Recent Ejaculation
Ejaculation may temporarily increase PSA. Some clinicians recommend avoiding ejaculation for one or two days before testing.
The National Cancer Institute advises avoiding activities that may increase PSA for two days before a test, unless your healthcare provider gives different instructions.
Cycling and Vigorous Exercise
Cycling may temporarily affect PSA in some people because a bicycle seat can place pressure on the prostate. Research results have not been completely consistent.
It may be reasonable to avoid cycling and vigorous exercise for approximately 48 hours before testing, particularly if you have previously had a borderline result. Follow the instructions from the clinician or laboratory ordering the test.
Recent Urologic Procedures
A prostate biopsy, cystoscopy, urinary catheterization, or another procedure involving the prostate or urinary tract may temporarily increase PSA.
A prostate biopsy can affect the result for several weeks. Tell the clinician when the procedure occurred before scheduling another PSA test.
Testosterone Therapy
Testosterone and other medicines that increase testosterone levels may raise PSA in some people. Anyone using testosterone therapy should tell the clinician interpreting the test.
Medications That Can Lower PSA
Some medications may lower PSA and make the result appear less concerning than it would otherwise be.
The most important examples are:
- Finasteride
- Dutasteride
These 5-alpha-reductase inhibitors are commonly prescribed for BPH. Finasteride may also be used for hair loss.
A clinician may need to adjust the interpretation of PSA in someone taking one of these medications. Never stop a prescribed medicine simply to change a laboratory result. Provide the clinician with a complete list of prescription medicines, nonprescription products, and supplements.
How to Prepare for a PSA Blood Test
Preparation requirements may vary. Follow the instructions from your doctor or testing laboratory.
Common recommendations include:
- Avoid ejaculation for approximately 48 hours before the test.
- Avoid vigorous cycling or activities that put pressure on the prostate for approximately 48 hours.
- Tell your doctor about urinary symptoms, fever, infection, or pelvic pain.
- Report any recent prostate biopsy, cystoscopy, catheterization, or urinary procedure.
- Provide a complete medication and supplement list.
- Ask whether the PSA blood sample should be drawn before a digital rectal examination.
- Do not stop finasteride, dutasteride, testosterone, or another prescribed medication without medical advice.
If you have an active prostate or urinary infection, the clinician may postpone testing until the condition has resolved.
What Happens After a High PSA Result?
A single high PSA result does not always lead directly to a biopsy.
The AUA/SUO Early Detection of Prostate Cancer Guideline, amended in 2026, recommends repeating a newly elevated PSA before proceeding to a secondary biomarker test, imaging, or biopsy.
1. The PSA Test May Be Repeated
For an abnormal screening result in a person without symptoms, the National Cancer Institute states that a doctor may repeat PSA in approximately six to eight weeks.
Repeating the test can help determine whether the elevation is persistent or was caused by normal laboratory variation or a temporary factor.
The timing may be different when:
- PSA is extremely high
- Symptoms suggest an infection
- A prostate examination is abnormal
- A recent procedure may have affected the result
- The clinician believes further testing should not be delayed
2. Your Medical History Is Reviewed
The clinician may ask about:
- Previous PSA results
- Urinary symptoms
- Fever, pain, or infection
- Recent ejaculation or cycling
- Recent procedures
- BPH or prostatitis
- Family history
- Ancestry
- Genetic test results
- Medicines and supplements
The pattern over time can be more informative than one isolated number.
3. A Digital Rectal Examination May Be Performed
During a digital rectal examination, a clinician feels the prostate through the rectal wall to check for firmness, asymmetry, lumps, or other abnormalities.
A DRE cannot rule prostate cancer in or out. However, it may add useful information when PSA is elevated.
4. Additional Blood or Urine Tests May Be Considered
Tests that may help refine the probability of clinically significant cancer include:
- Percent-free PSA
- Prostate Health Index
- 4Kscore
- IsoPSA
- ExoDx Prostate test
- SelectMDx
- Other validated risk-assessment tools
These tests are not necessary for everyone. Their purpose is often to help decide whether MRI or biopsy is appropriate.
5. Prostate MRI May Be Recommended
A multiparametric MRI can identify areas of the prostate that appear suspicious.
MRI findings may help doctors:
- Estimate the risk of clinically significant cancer
- Choose whether a biopsy is needed
- Target suspicious areas during biopsy
- Reduce some unnecessary procedures
MRI cannot provide a definitive diagnosis by itself. A suspicious finding usually requires interpretation alongside PSA, prostate size, examination findings, and other risk factors.
6. A Prostate Biopsy May Be Needed
A biopsy removes small samples of prostate tissue for examination under a microscope.
Biopsy may be considered when the overall risk remains concerning based on PSA, examination findings, biomarkers, imaging, family history, and other factors.
A high PSA alone is not an automatic biopsy order. The decision should be made through shared decision-making after reviewing the potential benefits, limitations, and complications.
Percent-Free PSA and High Results
PSA circulates in the blood in two primary forms:
- PSA attached to blood proteins
- Free, unattached PSA
The percent-free PSA compares free PSA with total PSA.
People with prostate cancer tend to have a lower percentage of free PSA than people with benign prostate conditions. Doctors may use this test when total PSA is between 4 and 10 ng/mL.
Many clinicians recommend considering biopsy more strongly when percent-free PSA is 10% or lower. A biopsy may also be considered when percent-free PSA is between 10% and 25%.
These are not universal biopsy thresholds. The appropriate cutoff can change according to total PSA and other risk factors.
What Are PSA Velocity and PSA Density?
PSA Velocity
PSA velocity measures how quickly PSA changes over time.
A rising pattern may attract attention, but PSA velocity should not be used by itself to determine whether someone needs a biomarker test, MRI, or biopsy. Temporary inflammation and normal biological variation can also produce changes.
PSA Density
PSA density compares the PSA level with the volume of the prostate.
A larger prostate may naturally produce more PSA. PSA density attempts to account for prostate size by dividing PSA by prostate volume.
A higher PSA density may increase concern, but it remains one part of a broader risk assessment. Measuring prostate volume generally requires ultrasound or MRI.
When Should PSA Screening Begin?
Medical organizations do not all recommend the same starting age or screening schedule.
Screening should involve shared decision-making. That means reviewing the possible benefits, false-positive results, overdiagnosis, biopsy complications, treatment side effects, personal risk, life expectancy, and individual preferences.
| Organization | Current screening approach |
|---|---|
| AUA/SUO, amended 2026 | A baseline PSA may be offered at ages 45–50. Screening should be offered at ages 40–45 for people at increased risk. Regular screening every two to four years is recommended for many people ages 50–69, with personalization based on risk and health. |
| American Cancer Society | Discuss screening at age 50 for average-risk men expected to live at least 10 more years; age 45 for high-risk men; and age 40 for those at even higher risk. |
| USPSTF | Ages 55–69 should make an individual decision after discussing benefits and harms. Routine PSA screening is not recommended for age 70 and older. |
Increased-risk groups identified by the AUA include people with Black ancestry, relevant germline mutations, or a strong family history of prostate cancer.
The American Cancer Society recommends beginning the discussion at age 45 for Black men and men with a first-degree relative diagnosed before age 65. It recommends discussion at age 40 for men with more than one first-degree relative diagnosed at an early age.
The current USPSTF prostate cancer screening recommendation advises individual decision-making for ages 55–69 and recommends against routine PSA-based screening in men age 70 and older.
Screening After Age 70
An age-based PSA chart should not be interpreted as a recommendation that every older adult needs screening.
For people over 70, the possible benefit of finding a slow-growing cancer may be outweighed by the risks of false-positive results, biopsy complications, overdiagnosis, and treatment side effects.
Some healthy older adults may still discuss testing with their clinicians. The decision should account for overall health, life expectancy, prior PSA results, risk factors, and personal preferences—not age alone.
Benefits and Limitations of PSA Screening
PSA screening may identify prostate cancer before symptoms develop and before the disease has spread.
However, testing also has important limitations:
- PSA can be elevated without cancer.
- Cancer may be present when PSA is relatively low.
- Screening can identify slow-growing cancers that would never cause symptoms.
- False-positive results can create anxiety.
- Further evaluation may involve MRI, biomarker testing, or biopsy.
- Biopsy can cause pain, bleeding, and infection.
- Treatment may cause urinary, sexual, or bowel side effects.
The National Cancer Institute reports that approximately 6%–7% of men have a false-positive result during any individual screening round. Only about 25% of men biopsied because of an elevated PSA are found to have prostate cancer.
These limitations are why PSA screening is based on informed, shared decision-making instead of automatic testing for every person of a certain age.
Does the Age Chart Apply After Prostate Cancer Treatment?
No. The PSA levels chart by age is intended primarily for people who have a prostate and are being screened or evaluated for the first time.
It should not be used to interpret PSA after:
- Radical prostatectomy
- Radiation therapy
- Hormone therapy
- Focal prostate treatment
- A prostate cancer diagnosis
- Active surveillance
After prostate cancer treatment, doctors often expect much lower PSA values and use treatment-specific definitions of recurrence. Even a small increase may have a different meaning than it would in someone who has never been diagnosed.
Follow the monitoring schedule provided by the treating urologist or oncology team.
When Should You Contact a Doctor?
Schedule a medical appointment if:
- Your PSA is above the reference range shown on your laboratory report.
- PSA has risen significantly compared with an earlier test.
- A repeat test remains elevated.
- You have difficulty urinating.
- You urinate much more frequently than usual.
- Urination is painful.
- You notice blood in your urine or semen.
- You have persistent pelvic, hip, or back pain.
- You develop fever or chills with urinary symptoms.
- You have a strong family history and are unsure when screening should begin.
These symptoms do not necessarily indicate prostate cancer. BPH, urinary infection, prostatitis, bladder conditions, and other problems can cause similar symptoms. Medical evaluation can help identify the cause.
Frequently Asked Questions
What is a normal PSA level for a 50-year-old?
A commonly cited upper reference level for ages 50–59 is 3.5 ng/mL. However, some clinicians may investigate levels above 2.5 or 3.0 ng/mL depending on previous results, family history, ancestry, medications, examination findings, and overall risk.
The laboratory range and personal clinical context are more important than the chart alone.
What is a normal PSA level for a 60-year-old?
The traditional upper age-adjusted reference level for ages 60–69 is 4.5 ng/mL.
A 2022 meta-analysis reported a pooled upper reference value of 4.9 ng/mL for men in their 60s. Neither value should be treated as a universal cancer cutoff.
What is a normal PSA level for a 70-year-old?
A commonly cited upper reference level for ages 70–79 is 6.5 ng/mL.
Routine screening is not automatically recommended simply because a result falls below that number. Overall health, life expectancy, prior results, symptoms, and personal preferences should guide testing and follow-up.
Is a PSA level of 4 high?
A PSA of 4 ng/mL may be considered elevated, particularly in a younger adult. It may be within a commonly cited age-adjusted range for some older adults.
A result of 4 does not diagnose cancer. A clinician may repeat the test, review temporary causes, perform an examination, or order additional risk-assessment tests.
Can an enlarged prostate cause a PSA of 10?
A substantially enlarged prostate can raise PSA, and noncancerous conditions may sometimes produce levels around or above 10 ng/mL.
However, PSA above 10 is associated with a significantly higher probability of prostate cancer and should receive timely medical evaluation. It should not be assumed to be caused only by BPH.
How long should I avoid ejaculation before a PSA test?
Many clinicians recommend avoiding ejaculation for approximately 48 hours before testing because it may temporarily increase PSA.
Follow the instructions from your healthcare provider or laboratory, especially if your previous result was borderline.
Can PSA go back down after being high?
Yes. PSA may decrease when a temporary cause resolves, such as inflammation, infection, recent ejaculation, cycling, or a recent prostate procedure.
Because PSA can vary, clinicians often repeat a newly elevated screening result before recommending biomarkers, imaging, or biopsy. A falling PSA does not eliminate the need for follow-up when other risk factors remain concerning.
Conclusion
A PSA levels chart by age can help you understand how results often change across different decades of life. Commonly cited upper reference levels are 2.5 ng/mL for ages 40–49, 3.5 for ages 50–59, 4.5 for ages 60–69, and 6.5 for ages 70–79.
These numbers are not universal definitions of normal, and they cannot diagnose or rule out prostate cancer.
The most useful interpretation combines your current result with previous PSA levels, age, prostate size, symptoms, family history, ancestry, medications, overall health, and additional test findings. Discuss an abnormal or changing result with a healthcare professional rather than trying to interpret the number by itself.
This content is for informational purposes only and not medical advice.
References
- National Cancer Institute: Prostate-Specific Antigen Test
- American Urological Association and Society of Urologic Oncology: Early Detection of Prostate Cancer Guideline, Amended 2026
- American Cancer Society: Prostate Cancer Screening Tests
- American Cancer Society: Recommendations for Prostate Cancer Early Detection
- U.S. Preventive Services Task Force: Prostate Cancer Screening
- PubMed: Age-Adjusted Reference Values for Prostate-Specific Antigen
- PubMed: Serum Prostate-Specific Antigen in a Community-Based Population