
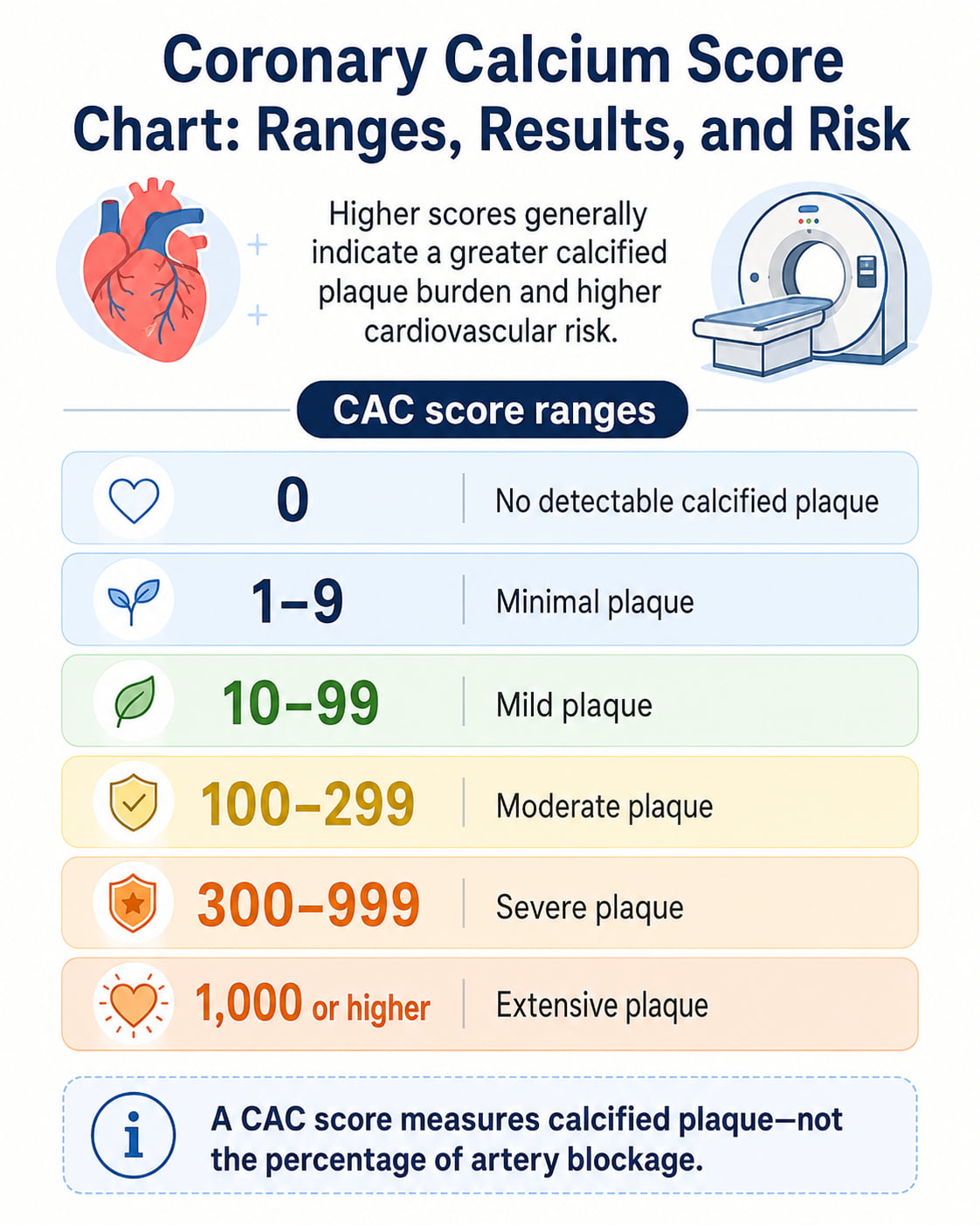
A coronary calcium score of 0 means no calcified plaque was detected, while any score above 0 indicates some calcified coronary atherosclerosis. Higher scores generally reflect a greater plaque burden and higher future cardiovascular risk.
A coronary artery calcium test can help clarify heart risk when cholesterol levels, blood pressure, age, family history, and other factors do not provide a clear treatment decision. However, the score does not measure the percentage of artery blockage and cannot predict exactly whether or when a heart attack will occur.
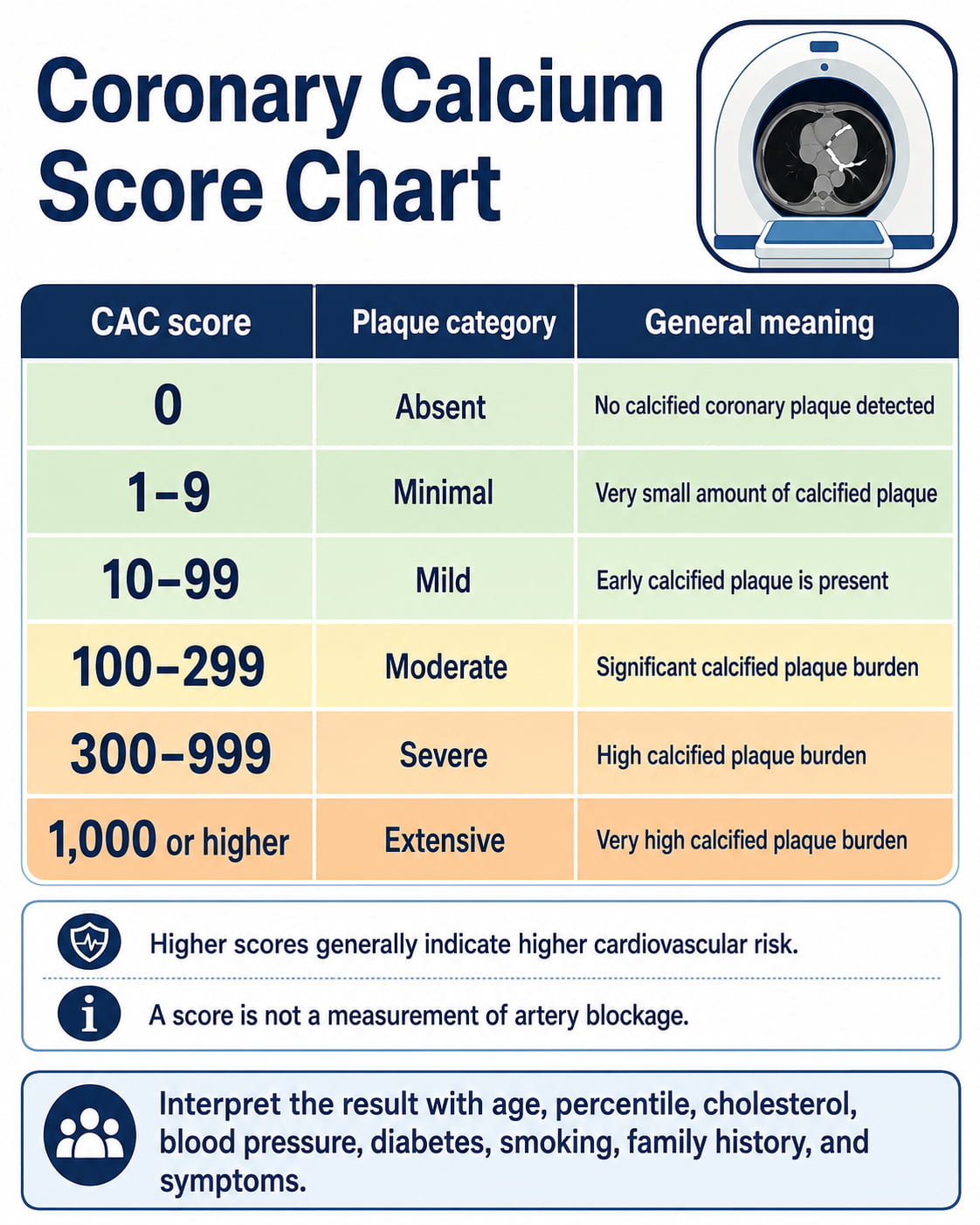
The latest American Heart Association chart divides results into six ranges: 0, 1–9, 10–99, 100–299, 300–999, and 1,000 or higher. Your result should always be interpreted with your symptoms, medical history, cholesterol levels, other risk factors, and calcium score percentile.
Coronary Calcium Score Chart
The following coronary calcium score chart is based on current patient guidance from the American Heart Association. The treatment descriptions are general discussion points—not instructions to start or change medication without a clinician.
| CAC score | Plaque category | General meaning | Common next discussion |
|---|---|---|---|
| 0 | Absent | No calcified coronary plaque was detected. Short-term cardiovascular risk is generally lower, but risk is not zero. | Continue prevention. Some people may be able to defer cholesterol medication after reviewing other risk factors. |
| 1–9 | Minimal | A very small amount of calcified plaque is present. This confirms early coronary atherosclerosis. | Reinforce healthy habits and review age, LDL cholesterol, smoking, diabetes, family history, and percentile. |
| 10–99 | Mild | Early-stage calcified plaque is present. Risk is higher than with a score of 0. | Discuss cholesterol-lowering therapy and management of all modifiable risk factors. |
| 100–299 | Moderate | A significant amount of calcified plaque is present. Cardiovascular risk is meaningfully elevated. | Statin therapy is generally recommended unless there is a specific reason not to use it. |
| 300–999 | Severe | The coronary plaque burden is high, with substantially elevated cardiovascular risk. | Intensive LDL lowering and close clinical follow-up are generally appropriate. |
| 1,000 or higher | Extensive | The calcified plaque burden and estimated cardiovascular risk are very high. | Intensive management of LDL cholesterol and all other modifiable risk factors is recommended. |
A score of 400, for example, falls in the severe 300–999 category. A score of 1,200 falls in the extensive category.
These ranges describe calcified plaque burden. They are not percentages, stages of artery blockage, or guarantees of a future cardiovascular event.
What Is a Coronary Calcium Score?
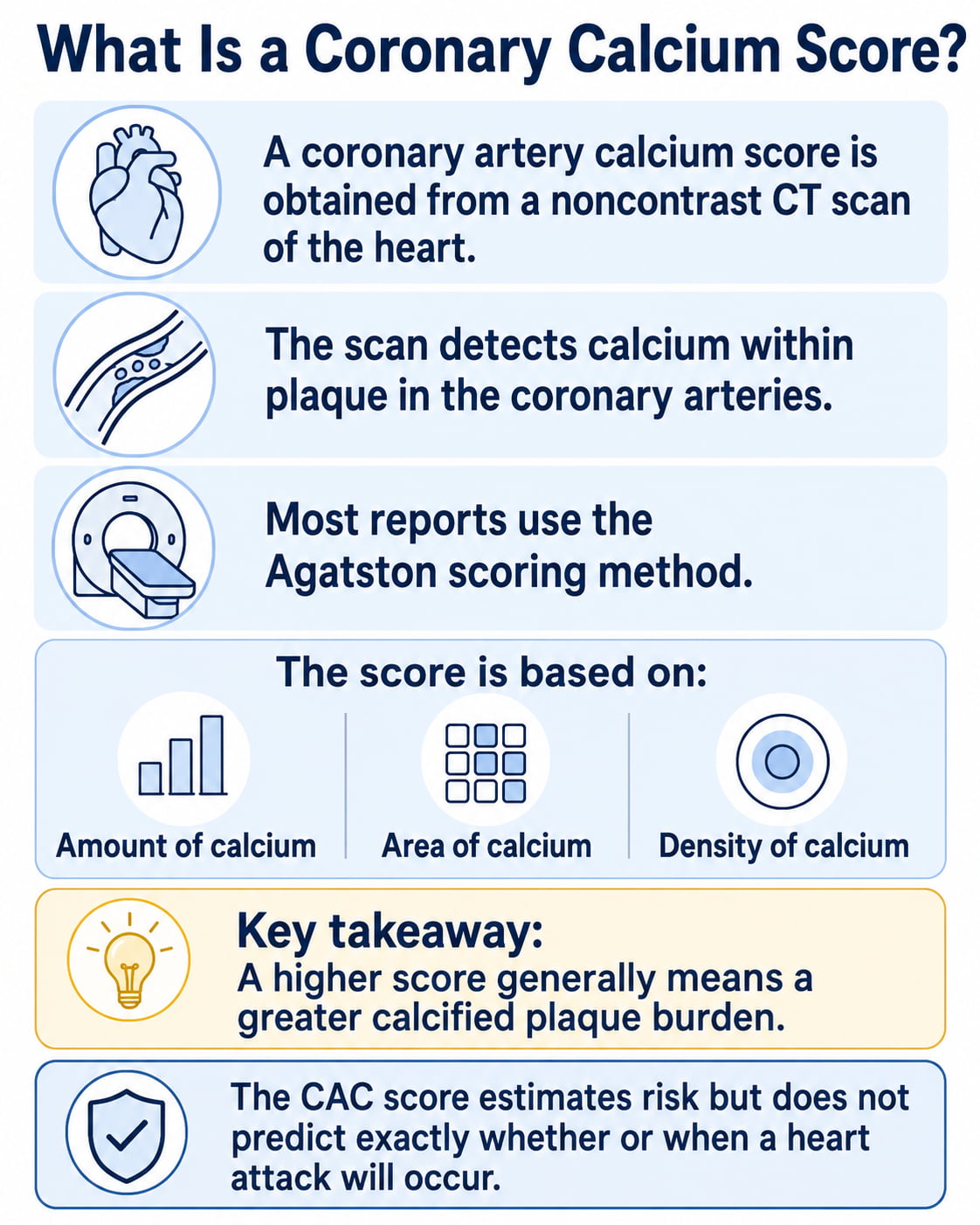
A coronary artery calcium, or CAC, score is produced by a specialized noncontrast CT scan of the heart. The scan looks for calcium within plaque in the walls of the coronary arteries—the vessels that supply blood to the heart muscle.
Most reports use the Agatston scoring method. It calculates a score based on the area and density of the calcium detected in the coronary arteries. The result may be shown as a plain number or as Agatston units, abbreviated AU.
In general:
- More calcified plaque produces a higher score.
- A higher score is associated with a higher risk of coronary heart disease and cardiovascular events.
- The score must be combined with other health information to estimate personal risk.
The test is mainly a risk-assessment tool for people without symptoms. It is not the same as coronary CT angiography, an exercise stress test, or an invasive coronary angiogram.
How to Interpret Each Coronary Calcium Score Range
CAC Score of 0: No Detectable Calcified Plaque
A score of 0 means the scan did not find measurable calcified plaque in the coronary arteries. This is usually reassuring and is associated with a lower short-term cardiovascular risk than a positive result.
However, a zero score does not mean:
- Your heart attack risk is zero.
- Your arteries contain no plaque of any kind.
- You can ignore cholesterol, blood pressure, smoking, or diabetes.
- Chest pain can safely be dismissed.
- You will never need preventive medication.
A standard calcium scan does not reliably identify noncalcified, or “soft,” plaque. This may be especially relevant in younger adults, who can have coronary plaque before much of it becomes calcified.
A score of 0 may allow medication to be deferred in selected people who do not have major risk factors. Diabetes, cigarette smoking, very high cholesterol, and a strong family history can still support treatment even when the CAC score is 0.
CAC Score of 1–9: Minimal Plaque
A result between 1 and 9 confirms that a small amount of calcified coronary plaque is present. The absolute amount is low, but it is not the same as having no plaque.
This range may be more important in a younger adult because any measurable calcium can be unusual at a younger age. The percentile and complete risk profile help determine whether medication is reasonable.
The 2026 dyslipidemia guideline generally supports discussing moderate-intensity statin therapy when a score of 1–99 is below the 75th percentile, although the final decision should reflect individual risk, preferences, medication tolerance, and existing health conditions.
CAC Score of 10–99: Mild Plaque
A score between 10 and 99 indicates mild calcified plaque burden. This confirms coronary atherosclerosis even if the person feels well and has no symptoms.
Clinicians commonly review:
- The score percentile
- LDL and non-HDL cholesterol
- Blood pressure
- Diabetes or chronic kidney disease
- Tobacco exposure
- Family history of early cardiovascular disease
- Lipoprotein(a), when available
- The estimated 10- and 30-year cardiovascular risk
Medication decisions should not be based on the calcium score alone. A 45-year-old and a 75-year-old with the same absolute score may have different percentiles and different overall risk profiles.
CAC Score of 100–299: Moderate Plaque
A score between 100 and 299 means a significant amount of calcified plaque is present. This range is associated with a clearly higher cardiovascular risk than a score below 100.
Current guidance generally supports LDL-lowering therapy for this range. The 2026 guideline recommends aiming for at least a 50% LDL-C reduction and an LDL-C level below 70 mg/dL when the CAC score is 100–999 or the result is at or above the 75th standardized percentile. The exact medication and target should be determined with a clinician.
A score in this range does not automatically mean a coronary artery is severely narrowed. It shows the total calcified plaque burden—not the percentage of blood-flow obstruction.
CAC Score of 300–999: Severe Plaque
A score from 300 through 999 indicates severe calcified plaque burden and a substantially elevated cardiovascular risk.
The 2026 guideline supports intensive LDL lowering in this group. It considers further intensification toward an LDL-C goal below 55 mg/dL reasonable, using the appropriate statin intensity and, when needed, additional clinician-prescribed LDL-lowering medication.
This result usually calls for a detailed review of:
- LDL and non-HDL cholesterol
- Blood pressure control
- Blood sugar
- Tobacco use
- Exercise and dietary habits
- Kidney function
- Family history
- Symptoms that could indicate reduced blood flow to the heart
A high score alone does not determine whether a stress test, CT angiogram, stent, or bypass operation is needed. Those decisions depend on symptoms, functional testing, anatomy, and other clinical findings.
CAC Score of 1,000 or Higher: Extensive Plaque
A score of at least 1,000 indicates an extensive calcified plaque burden and very high cardiovascular risk.
Current guidance recommends intensive LDL-lowering therapy, aiming for at least a 50% LDL-C reduction and an LDL-C level below 55 mg/dL. Reaching this level may require more than one medication, but medication choices must be individualized by a qualified clinician.
An extensive score requires proactive medical follow-up. However, it does not automatically mean an immediate heart attack is occurring or that every coronary artery is critically blocked.
2026 CAC Score and LDL Cholesterol Guidance
The American College of Cardiology and American Heart Association published updated dyslipidemia guidance on March 13, 2026, expanding the role of CAC scoring in cardiovascular risk assessment.
The guideline recommends considering both the absolute score and standardized percentile. The following is a simplified summary for adults with subclinical coronary atherosclerosis who have not already experienced a clinical cardiovascular event.
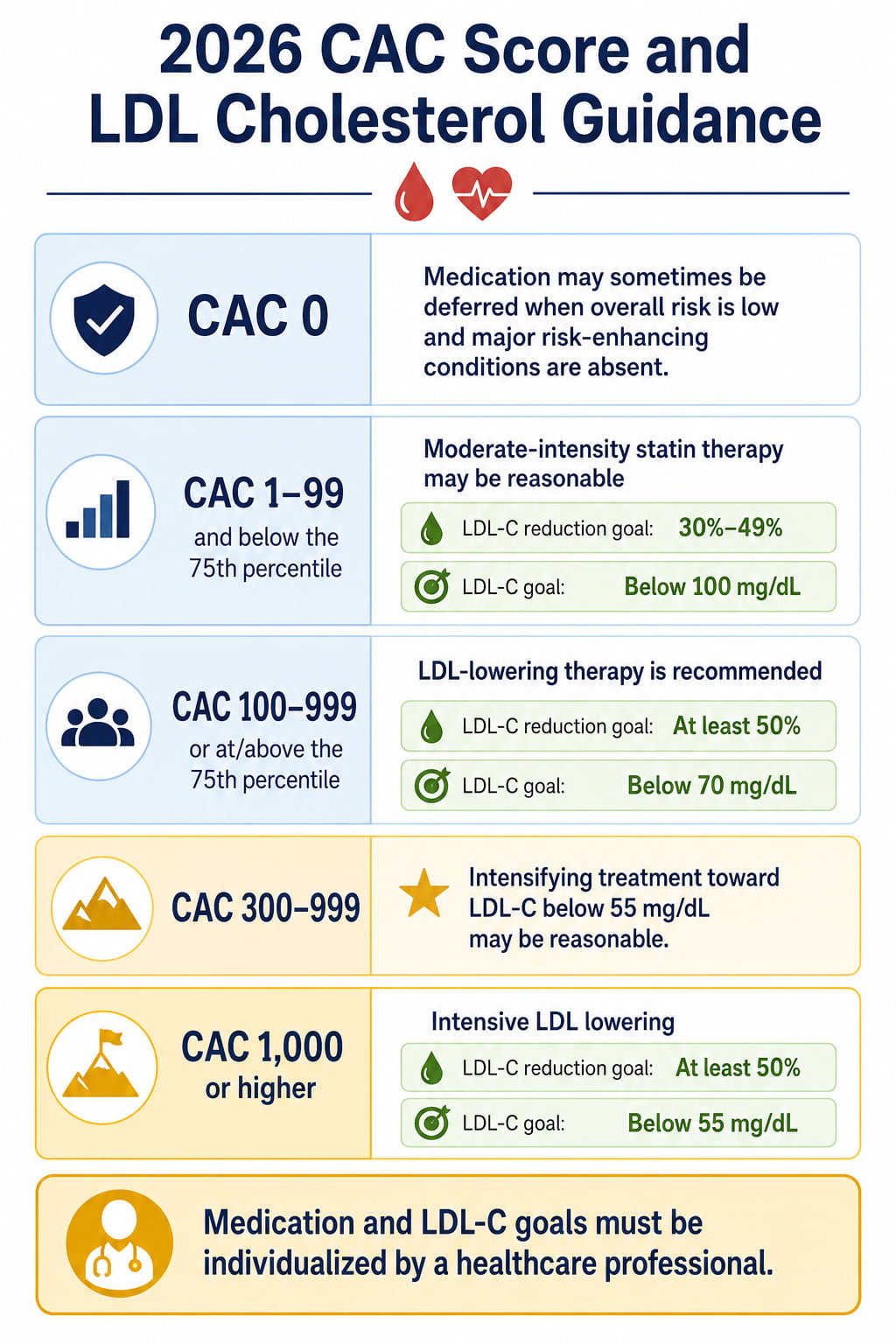
| CAC result | Simplified guideline direction |
|---|---|
| 0 | Medication may sometimes be deferred when overall risk is low and no important risk-enhancing conditions are present. |
| 1–99 and below the 75th percentile | Moderate-intensity statin therapy is considered reasonable; guideline goals include a 30%–49% LDL-C reduction and LDL-C below 100 mg/dL. |
| 100–999 or at/above the 75th percentile | LDL-lowering therapy is recommended, with at least a 50% LDL-C reduction and LDL-C below 70 mg/dL. |
| 300–999 | Intensifying therapy toward LDL-C below 55 mg/dL is considered reasonable. |
| 1,000 or higher | Intensive LDL lowering is recommended, with at least a 50% reduction and LDL-C below 55 mg/dL. |
These targets do not replace personalized care. People with known coronary disease, a previous heart attack, stroke, stent, or bypass surgery are generally managed under secondary-prevention recommendations rather than CAC-based primary-prevention guidance.
Do not start a statin, aspirin, or another cardiovascular medication based only on an online chart. A clinician should review possible benefits, side effects, interactions, bleeding risk, and alternative options.
What Is a CAC Percentile?
An absolute CAC score shows how much calcified plaque was measured. A percentile shows how the result compares with people of a similar age and demographic profile.
A result at the 75th percentile means the score is as high as or higher than the scores of approximately 75% of the comparison group.
The current guideline gives both numbers prognostic importance. A score below 100 may still be concerning when it is at or above the 75th percentile.
The Multi-Ethnic Study of Atherosclerosis provides a CAC reference tool with estimates based on age, sex, and race or ethnicity. Its reference data are based on adults ages 45–84 who were free of clinical cardiovascular disease and treated diabetes at baseline. The tool is useful for context, but it does not independently determine whether someone is high risk.
Example of Why Percentile Matters
Consider two hypothetical people who both have a score of 40:
- In a younger person, 40 may be unusually high compared with peers.
- In an older person, 40 may be at a lower percentile, although it still confirms calcified plaque.
The younger person may therefore have a lower absolute score but a more concerning age-relative result.
What Is a Normal Calcium Score by Age?
There is no single “normal” positive calcium score for each age.
Aging makes coronary calcium more common, but a positive score still represents calcified atherosclerotic plaque. A score should not be considered harmless simply because similar scores are common among older adults.
A practical interpretation is:
- CAC 0: No calcified plaque detected.
- CAC above 0: Some calcified plaque is present.
- Higher absolute score: Greater measured plaque burden.
- Higher percentile: More calcium than most comparable people.
- Absolute score plus percentile: Provides better context than either number alone.
Age does not cancel the meaning of a positive result. It helps clinicians interpret how unusual that result is and how aggressively risk factors may need to be managed.
How Much Does Cardiovascular Risk Rise With CAC?
Long-term data from the Multi-Ethnic Study of Atherosclerosis show a graded relationship between CAC and cardiovascular events.
In an analysis of 6,814 adults without known cardiovascular disease:
- Ten-year ASCVD event rates ranged from approximately 1.3% to 5.6% among people with CAC 0.
- Event rates ranged from approximately 13.1% to 25.6% among those with CAC above 300.
- A score of at least 100 was associated with a ten-year event rate above 7.5% across the demographic groups studied.
- Each doubling of the CAC score was associated with an approximately 14% relative increase in ASCVD risk after adjustment for standard risk factors.
These are population-level findings, not guaranteed outcomes for an individual. Risk varied across age, sex, and racial or ethnic groups.
Does a Calcium Score Show Artery Blockage?
No. A CAC score does not show the percentage of artery blockage.
A score of 100 does not mean an artery is 100% blocked. A score of 400 does not mean four arteries are blocked.
The number represents the amount and density of calcified plaque across the coronary arteries. It does not directly measure the width of the channel through which blood flows.
RadiologyInfo.org explains that a calcium scan identifies calcified plaque but cannot reliably evaluate noncalcified plaque or determine how severely a coronary artery has narrowed. Other testing may be needed when the clinical question involves stenosis or blood flow.
What a Coronary Calcium Scan Cannot Tell You
A standard CAC scan cannot:
- Show all noncalcified plaque.
- Measure the exact percentage of artery narrowing.
- Show whether the heart muscle receives enough blood during exercise.
- Identify which plaque, if any, may rupture.
- Predict the exact timing of a heart attack.
- Determine by itself whether a stent or bypass surgery is needed.
- Rule out heart disease in someone with concerning symptoms.
- Replace a complete cardiovascular evaluation.
A person can have a relatively low CAC score and still have clinically important noncalcified plaque. Conversely, a person can have a high total score without a critical blockage in one particular artery.
Who Should Consider a Coronary Calcium Scan?
CAC testing is most useful when the result could change a prevention decision.
The 2026 guideline recommends selective use particularly for:
- Men age 40 or older
- Women age 45 or older
- People with borderline or intermediate estimated ten-year cardiovascular risk
- People uncertain about beginning statin therapy
- People whose risk remains unclear after reviewing conventional risk factors
- People who want more individualized information before making a long-term prevention decision
The guideline now uses the AHA PREVENT equations to estimate ten- and thirty-year cardiovascular risk in appropriate adults. The major ten-year categories are:
| PREVENT-ASCVD category | Ten-year estimated risk |
|---|---|
| Low | Below 3% |
| Borderline | 3% to below 5% |
| Intermediate | 5% to below 10% |
| High | 10% or higher |
CAC is most useful when someone is near a treatment threshold and the result could reasonably change the plan. It should not be ordered automatically simply because a person has reached a certain age.
Who May Not Benefit From CAC Testing?
A routine calcium scan may provide limited value when:
- Cardiovascular risk is already very low.
- The need for treatment is already clear.
- The person already has diagnosed coronary artery disease.
- There is a history of heart attack, coronary stent, or bypass surgery.
- The person has chest pain or other symptoms requiring diagnostic testing.
- The result would not change the treatment plan.
- Repeated scanning would add radiation without changing care.
People with symptoms need a symptom-focused medical evaluation. A screening calcium scan is not designed to determine whether current chest pain is caused by reduced blood flow.
What Happens During a Coronary Calcium Scan?
A standard CAC scan is quick and noninvasive.
The usual process includes:
- Small electrodes are attached to the chest to record the heartbeat.
- The person lies on a table that moves through the CT scanner.
- The scanner takes images synchronized with the heartbeat.
- The technologist may ask the person to hold their breath briefly.
- Computer software calculates the calcium score.
No contrast dye or injection is normally needed. There is no recovery period, and most people can resume their usual activities immediately.
The scanning appointment often takes approximately 10–15 minutes, although the actual image collection may take only a few minutes.
Radiation and Safety
A CAC scan uses a relatively low dose of ionizing radiation. The exact dose varies with the scanner, imaging protocol, body size, and facility.
Because radiation is involved:
- The test should be performed when the expected information is useful.
- Unnecessary repeat scans should be avoided.
- Anyone who is pregnant or may be pregnant should tell the clinician and imaging center beforehand.
- Benefits and limitations should be discussed before testing.
The test does not leave radiation in the body.
How Much Does a Coronary Calcium Scan Cost?
Insurance coverage varies. Some health plans cover CAC testing, while others classify it as an elective screening test.
An uncovered scan generally costs approximately $50 to $250. Prices can vary by imaging center and location.
Before scheduling, ask the facility:
- What is the total self-pay price?
- Does the price include the radiologist’s interpretation?
- Is a clinician’s order required?
- Will insurance be billed?
- Are follow-up services charged separately?
How Often Should a Calcium Scan Be Repeated?
Repeat testing is not needed every year.
When the initial score is 0, reassessment may be considered in approximately 3–7 years, depending on the person’s risk factors and whether a new result would change care.
A similar interval may sometimes be discussed for a minimal result. However, if a high score has already led to intensive preventive treatment, repeating the scan generally does not change the care plan.
CAC commonly increases over time, and statin therapy may affect plaque composition and calcium density. For this reason, a rising Agatston score does not always provide a simple measurement of whether treatment is succeeding or failing.
Follow cholesterol, blood pressure, blood sugar, tobacco use, activity, and medication adherence rather than relying on repeat CT scans alone.
What to Do After Receiving Your CAC Result
1. Review the Complete Report
Look for:
- Total Agatston score
- Calcium score percentile
- Calcium in individual coronary arteries
- Incidental findings outside the coronary arteries
- The radiologist’s interpretation
- Recommended follow-up
Do not interpret the number without reading the rest of the report.
2. Discuss Your Overall Risk
Bring recent information about:
- LDL, HDL, and triglycerides
- Blood pressure
- A1C or fasting blood glucose
- Smoking or vaping
- Kidney function
- Family history
- Current medications
- Exercise habits
- Any chest discomfort or shortness of breath
The score becomes more useful when combined with these factors.
3. Ask About an LDL-C Goal
The appropriate LDL target may depend on the score, percentile, age, medical conditions, and whether clinical cardiovascular disease is already present.
Useful questions include:
- What LDL-C goal is appropriate for me?
- Is a statin recommended?
- What percentage LDL reduction should we aim for?
- When should my cholesterol be rechecked?
- Are additional medications needed if the goal is not reached?
4. Strengthen Heart-Healthy Habits
Regardless of the score, prevention generally includes:
- Avoiding tobacco and secondhand smoke
- Eating more vegetables, fruits, legumes, whole grains, nuts, and other minimally processed foods
- Choosing unsaturated fats in place of trans fats and excess saturated fat
- Limiting highly processed foods, excess sodium, and added sugar
- Completing at least 150 minutes of moderate activity or 75 minutes of vigorous activity weekly when medically appropriate
- Including muscle-strengthening activities
- Managing blood pressure, blood sugar, and cholesterol
- Getting approximately seven to nine hours of sleep
- Taking prescribed medication consistently
These steps support cardiovascular health but do not physically remove a high CAC score.
5. Do Not Start Aspirin on Your Own
Aspirin can increase bleeding risk. A high calcium score may influence an aspirin discussion in selected patients, but it does not automatically make aspirin safe or appropriate.
Do not start daily aspirin or change cholesterol medication without professional guidance.
When to Seek Urgent Medical Care
A CAC score is not an emergency test. However, symptoms may require immediate care regardless of the score.
Seek emergency medical help for possible heart attack symptoms, such as:
- New pressure, squeezing, fullness, or pain in the chest
- Pain spreading to the arm, shoulder, jaw, neck, back, or upper abdomen
- Shortness of breath
- Cold sweating
- Sudden nausea
- Faintness or severe lightheadedness
- Sudden unexplained weakness
Do not wait for a routine calcium scan appointment when these symptoms occur.
Frequently Asked Questions
What is considered a good coronary calcium score?
A score of 0 is the most reassuring result because no calcified coronary plaque was detected. It does not eliminate all cardiovascular risk or rule out noncalcified plaque.
Is a calcium score of 100 high?
A score of 100 is in the moderate plaque category under the current chart. It generally supports LDL-lowering treatment and a detailed review of cardiovascular risk factors.
What does a calcium score of 300 mean?
A score of 300 marks the beginning of the severe category in the current chart. It reflects a high plaque burden and substantially elevated risk. Intensive prevention and close follow-up are generally appropriate.
What does a calcium score of 400 mean?
A score of 400 falls within the severe 300–999 range. It does not mean an artery is 400% blocked or that a stent is automatically required. Further decisions depend on symptoms and the complete medical evaluation.
Can you have heart disease with a calcium score of 0?
Yes. A score of 0 excludes detectable calcified plaque, not every form of coronary disease. Noncalcified plaque, coronary microvascular disease, or other heart conditions may still be present.
Does a high calcium score mean I need a stent?
Not by itself. Stents are generally used to address clinically important narrowing or acute coronary problems—not simply a high total calcium score. Symptoms, coronary anatomy, blood-flow testing, and overall clinical findings guide the decision.
Can a coronary calcium score go down?
CAC scores usually do not decrease substantially because existing calcium generally remains visible. Prevention focuses on reducing future cardiovascular events and slowing disease progression rather than making the score return to zero.
Conclusion
A coronary calcium score chart provides a practical way to understand calcified coronary plaque burden. A score of 0 is reassuring but does not eliminate all risk. Scores of 1–99 confirm early plaque, 100–299 indicate moderate plaque, 300–999 indicate severe plaque, and 1,000 or higher represents an extensive burden.
The number should never be interpreted alone. Review the absolute score, percentile, cholesterol levels, blood pressure, blood sugar, tobacco exposure, family history, symptoms, and medication options with your healthcare professional. The most useful next step is not simply knowing the score—it is using the result to create an appropriate prevention plan.
This content is for informational purposes only and not medical advice.