
Pes anserine bursitis exercises are gentle stretches and strength moves (especially for the hamstrings, quads, and hips) that may help reduce irritation on the inner knee and support more comfortable walking and stairs.

Keeping the movements pain-free and progressive matters because pes anserine bursitis is often linked to overload and movement mechanics, and it typically responds well to conservative care like exercise and stretching programs, as explained by the Cleveland Clinic and summarized in clinical overviews from the NCBI Bookshelf.
If your inner knee pain is sharp, worsening, warm/red, or you have fever or sudden swelling, get medical advice. General bursitis guidance from the NHS recommends evaluation when symptoms are severe or not improving.
What Is Pes Anserine Bursitis
Pes anserine bursitis is irritation of a small fluid-filled sac on the inside of the knee, near where three tendons attach. It often causes tenderness and pain on the inner knee, especially with stairs, getting up from a chair, or repetitive bending.
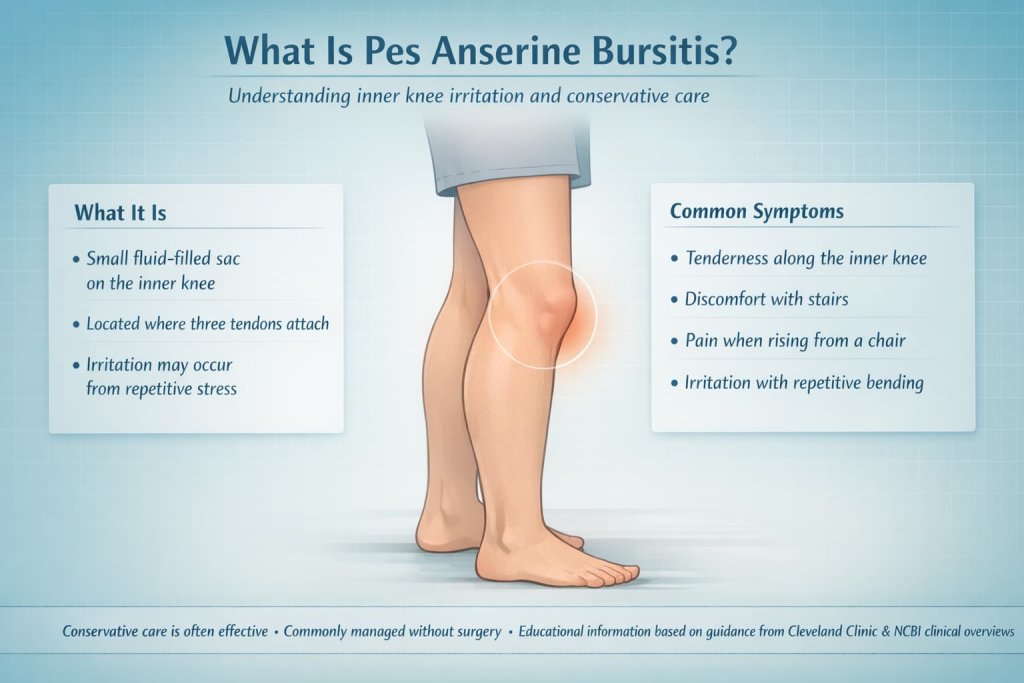
The Cleveland Clinic notes that conservative care is typically effective, and the NCBI Bookshelf describes it as a condition commonly managed without surgery.
Who Should Be Careful Before Starting These Exercises?
Pes anserine bursitis exercises are generally safe, but some people should get medical guidance before starting.
Be cautious if you have:
- Significant swelling, redness, warmth, or fever
- A recent knee injury or fall
- Knee locking, catching, or instability
- Severe pain with walking or weight-bearing
- Symptoms that are not improving after a few weeks
The Cleveland Clinic notes that inner knee pain can have multiple causes, so an accurate diagnosis is important before beginning a program.
10 Best Pes Anserine Bursitis Exercises to Reduce Inner Knee Pain
These 10 pes anserine bursitis exercises focus on gentle stretching and targeted strengthening to help reduce inner knee irritation. Follow this step-by-step plan to support knee stability, improve mobility, and return to daily activities safely.
1) Hamstring Stretch (Wall or Doorway)
Why it works: Tight hamstrings can increase stress near the pes anserine region. Gentle hamstring stretching is commonly included in rehabilitation plans to reduce excess tension along the inner knee.
How to do it:
- Lie on your back near a doorway or wall.
- Place the affected leg up the wall or doorframe with the knee comfortably straight.
- Keep the other leg flat on the floor.
- Hold 15–30 seconds, repeat 2–4 times.
Trainer Tip: Keep it gentle. You should feel a stretch in the back of the thigh, not sharp inner-knee pain.
2) Standing Calf Stretch
Why it works: Calf tightness can affect ankle motion and change knee loading during walking and stairs, which may aggravate inner-knee irritation.
How to do it:
- Face a wall, hands on wall at chest height.
- Step the sore-side leg back, heel down, knee straight.
- Lean forward until you feel a calf stretch.
- Hold 20–30 seconds, repeat 2–4 times.
Trainer Tip: Keep your back foot pointing straight ahead so the stretch stays in the calf, not the inner knee.
3) Quadriceps Stretch (Standing or Side-Lying)
Why it works: Quad flexibility supports smoother knee motion and may reduce compensations that irritate the medial knee.
How to do it:
- Stand holding a support, bend the knee and bring heel toward glute.
- Hold your ankle (or use a strap) and keep knees close together.
- Hold 20–30 seconds, repeat 2–4 times.
Trainer Tip: Keep your pelvis slightly tucked so you feel the stretch in the front thigh—not in the low back.
4) Heel Slides (Gentle Knee Range of Motion)
Why it works: Light range-of-motion keeps the knee moving without heavy compression, helping you stay active while symptoms calm down.
How to do it:
- Lie on your back with legs straight.
- Slowly slide your heel toward your butt until you feel a mild stretch.
- Slide back to straight.
- Do 10–15 reps, 1–2 sets.
Trainer Tip: Keep the movement smooth and small if the inner knee is sensitive.
5) Quad Sets (Isometric)
Why it works: Isometrics build knee support with minimal joint movement, which can be helpful during a flare. Conservative management approaches outlined in the NCBI Bookshelf include strengthening as symptoms allow.
How to do it:
- Sit or lie with the leg straight.
- Tighten the thigh muscle as if pushing the knee down into the floor.
- Hold 5–10 seconds, repeat 10–15 times.
Trainer Tip: Aim for a firm contraction without pain. If it pinches, reduce intensity.
6) Straight Leg Raise
Why it works: Strengthens the quads without deep knee bending, helping support walking and stair control.
How to do it:
- Lie on your back, one knee bent, sore-side leg straight.
- Tighten the quad, lift the straight leg to the height of the bent knee.
- Lower slowly.
- Do 8–12 reps, 2–3 sets.
Trainer Tip: Pause and reset your quad squeeze if you feel hip flexor strain.
7) Glute Bridge
Why it works: Hip strength helps control thigh position and may reduce repeated medial knee loading during daily movement.
How to do it:
- Lie on your back, knees bent, feet hip-width apart.
- Brace gently, squeeze glutes, lift hips until body forms a straight line from shoulders to knees.
- Pause briefly, then lower slowly.
- Do 8–12 reps, 2–3 sets.
Trainer Tip: Keep ribs down and press evenly through both feet.
8) Side-Lying Hip Abduction
Why it works: Strengthening the hip abductors can improve lower-limb alignment and reduce stress patterns that irritate the inner knee. The ChoosePT guide emphasizes strengthening surrounding muscles to reduce recurrence.
How to do it:
- Lie on your side, bottom knee bent for balance.
- Keep top leg straight, toes pointing forward.
- Lift the leg 12–18 inches, lower slowly.
- Do 10–15 reps, 2–3 sets.
Trainer Tip: Slightly rotate toes down if you feel it in the front of the hip.
9) Clamshells
Why it works: Builds hip external rotation control, which can help reduce knee collapse patterns that may aggravate medial knee structures.
How to do it:
- Lie on your side with hips and knees bent, feet together.
- Keep pelvis stacked; open the top knee without rolling back.
- Lower slowly.
- Do 12–20 reps, 2–3 sets.
Trainer Tip: Add a light band only if the movement stays pain-free.
10) Mini Squats or Wall Sits (Pain-Free Range)
Why it works: Adds functional quad and hip strength once symptoms calm down, preparing you for stairs and sit-to-stand movements.
How to do it:
- Stand with feet shoulder-width apart.
- Perform a small squat (about 0–45 degrees) while keeping knees tracking over toes.
- Return to stand.
- Do 8–12 reps, 2–3 sets.
Trainer Tip: If squats irritate your inner knee, shorten the range or switch to brief wall sits.
How Often Should You Do These Exercises?
Consistency is more important than intensity. Most conservative rehab programs suggest 3–5 days per week, depending on tolerance.
General guideline:
- Stretching: Daily or 5 days per week
- Isometrics (quad sets): Daily during flare-ups
- Strength exercises: 3–4 days per week
- Rest day between harder sessions if sore
Keep pain mild (0–3/10) and avoid sharp inner knee pain. Clinical overviews in the NCBI Bookshelf emphasize gradual load progression for recovery.
A Simple Weekly Progression
- Week 1 (Calm Phase): Hamstring stretch, calf stretch, heel slides, quad sets, light bridges.
- Week 2 (Build Phase): Add straight leg raises, clamshells, side-lying abduction.
- Week 3+ (Return to Function): Add mini squats or wall sits and gradually increase repetitions.
Progress one variable at a time—reps first, then sets, then resistance.
Safety Rules Before You Start Pes Anserine Bursitis Exercises
Use these simple rules to keep the program knee-friendly:
- Keep pain at a mild level (0–3/10). Stop if pain spikes or lingers worse the next day.
- Avoid deep knee bend positions early (deep squats, aggressive lunges, steep hills) if they flare symptoms.
- Move slow and controlled—no bouncing or forcing range.
- Start with stretching and isometrics, then add strengthening as symptoms settle.
- If you have knee osteoarthritis, recent injury, or persistent swelling, a physical therapist can tailor the plan, as recommended by the American Physical Therapy Association’s ChoosePT guide.
Common Mistakes That Slow Recovery
- Stretching aggressively into pain
- Returning to deep squats or heavy stair use too quickly
- Ignoring hip weakness
- Increasing activity load too fast after symptoms improve
When to See a Clinician
Consider evaluation if:
- Pain is worsening or not improving
- You have swelling, redness, warmth, or fever
- You experience locking, instability, or significant walking difficulty
General bursitis guidance from the NHS supports seeking care when symptoms are persistent or severe.
FAQs About Pes Anserine Bursitis Exercises
How long does pes anserine bursitis take to improve?
Many cases improve with conservative care. Recovery time varies depending on activity level, strength, and contributing conditions, as outlined in clinical reviews from the NCBI Bookshelf.
Should I completely rest my knee?
Complete rest may increase stiffness. Most guidance supports modifying aggravating activities while keeping gentle movement, according to the ChoosePT guide.
Are squats bad for pes anserine bursitis?
Deep squats may flare symptoms early. Short-range, pain-free squats can be introduced gradually.
What activities should I avoid?
Common triggers include repetitive stairs, hill running, and deep knee bending during a flare.
Do I need imaging?
Diagnosis is often clinical. Imaging may be considered if symptoms do not improve or if other knee conditions are suspected, as discussed in the NCBI Bookshelf.
Can pes anserine bursitis return?
Yes, especially if load management and strength deficits are not addressed. Strengthening surrounding muscles may help reduce recurrence risk.
Conclusion
Pes anserine bursitis exercises work best when they are gentle, consistent, and progressive. Start with flexibility and low-irritation strength work, then gradually build toward functional movements like mini squats. If symptoms persist or worsen, seek professional guidance to confirm the diagnosis and personalize your plan.
This content is for informational purposes only and not medical advice.